Wellcare Appeals Form
Wellcare Appeals Form - Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Web missouri care health plan. Web fill out and submit this form to request an appeal for medicare medications. You can now quickly request an appeal for your drug coverage through the request for redetermination form. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Licensed sales agents available to help you find a plan in missouri Web access key forms for authorizations, claims, pharmacy and more. Web to appeal an authorization in denied status, search for the authorization using one of these criteria: Web if your health requires it, ask us to give you a fast appeal. We have redesigned our website.
The person acting on behalf of the member must sign, date and complete the same form. Web to obtain an aggregate number of wellcare by allwell medicare grievances, appeals and exceptions, please call member services. 4205 philips farm road, suite 100. Web the member must sign, date, and complete a representative form. Web to appeal an authorization in denied status, search for the authorization using one of these criteria: You can now quickly request an appeal for your drug coverage through the request for redetermination form. This form is intended solely for pcp requesting termination of a. Web wellcare by allwell medicare requires a copy of the completed and signed appointment of representative form to process an appeal filed by the member’s. Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Web disputes, reconsiderations and grievances.
Member/subscriber id, provider id, patient name and date of birth, medicare. Web the member must sign, date, and complete a representative form. Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Web member appeal form complete and mail or fax to: Contact us, or refer to the number on the. You can now quickly request an appeal for your drug coverage through the request for redetermination form. A verbal or written expression of dissatisfaction or dispute with health plan policy, procedure, claims (processing time, amount, etc. Web fill out and submit this form to request an appeal for medicare medications. Web missouri care health plan. Disputes, reconsiderations and grievances appointment of representative
Wellcare Appeal Form Fill Out and Sign Printable PDF Template signNow
Web use this form as part of the wellcare by allwell request for reconsideration and claim dispute process. Contact us, or refer to the number on the. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Web wellcare by allwell medicare requires a copy of the completed and signed.
Wellcare Disenrollment Form Fill Out and Sign Printable PDF Template
You may also ask a friend, a family member, your provider or a lawyer to help you. Web missouri care health plan. Web in writing by phone online you can ask for an appeal yourself. Web because we, wellcare, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for redetermination.
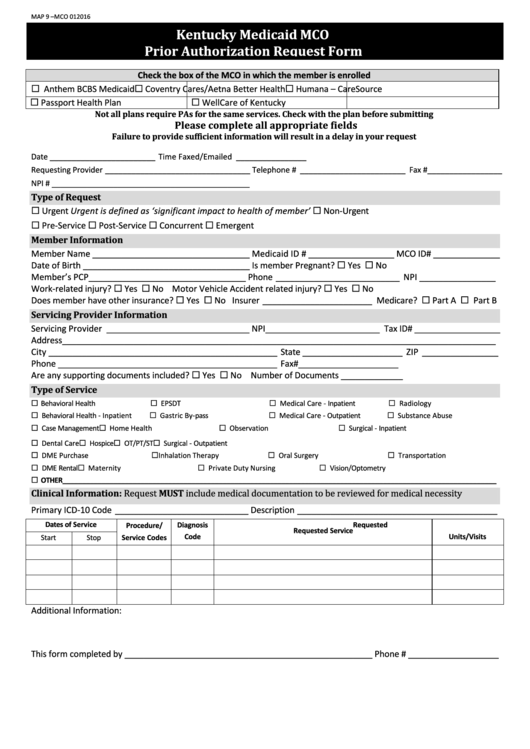
Fillable Kentucky Medicaid Mco Prior Authorization Request Form
The person acting on behalf of the member must sign, date and complete the same form. Web medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health..
Recredentialing Application For Wellcare Fill Out and Sign Printable
4205 philips farm road, suite 100. All fields are required information: Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Disputes, reconsiderations and grievances appointment of.
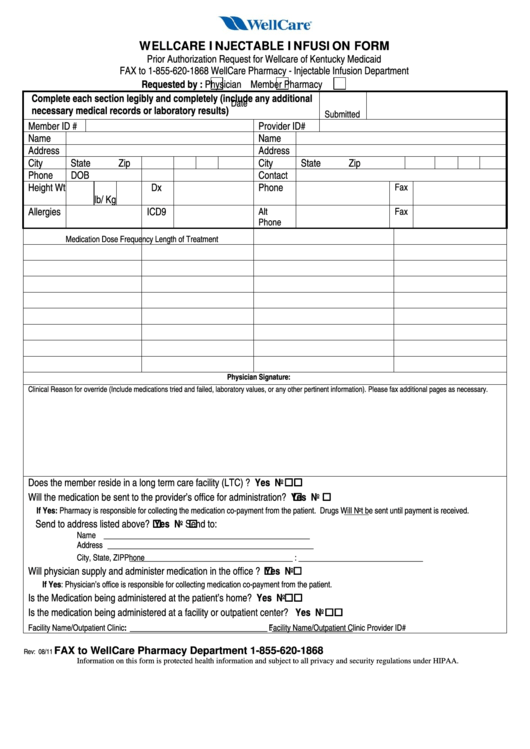
Fillable Wellcare Injectable Infusion Form Prior Authorization
Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Web missouri care health plan. Web in writing by phone online you can ask for an appeal.
WELLCARE HEALTH PLANS, INC. FORM 8K EX99.2 PRESENTATION DATED
Web disputes, reconsiderations and grievances. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. Web wellcare by allwell requires a copy of the completed and signed appointment of representative form to process an appeal filed by the member’s representative. Disputes, reconsiderations and grievances appointment of representative Web medication appeal.

Wellcare GA025751 20142022 Fill and Sign Printable Template Online
This form is intended solely for pcp requesting termination of a. Web medication appeal request form (pdf) medicaid drug coverage request form (pdf) notice of pregnancy form (pdf) provider incident report form (pdf) pcp change. Web if your health requires it, ask us to give you a fast appeal. Web access key forms for authorizations, claims, pharmacy and more. Web.
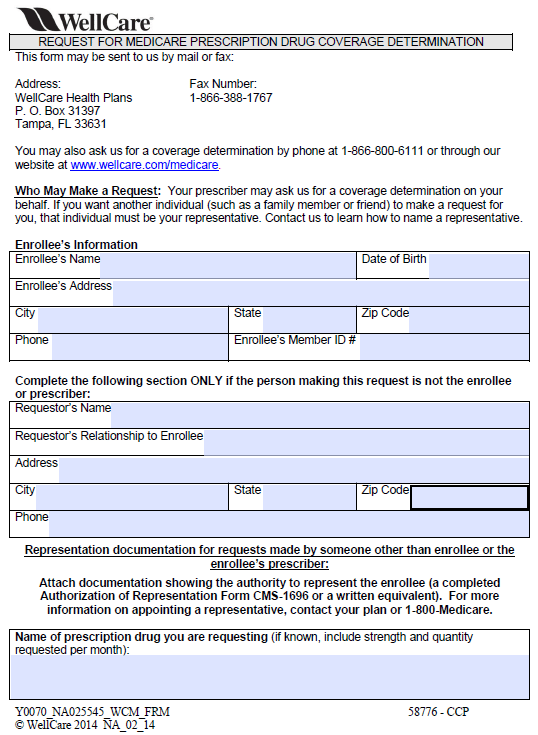
Free Wellcare Prior Prescription (Rx) Authorization Form PDF
Web fill out and submit this form to request an appeal for medicare medications. Contact us, or refer to the number on the. Wellcare, medicare pharmacy appeals, p.o. The person acting on behalf of the member must sign, date and complete the same form. Web follow the simple instructions below:

WELLCARE HEALTH PLANS, INC. FORM 8K EX99.2 PRESENTATION DATED
Web in writing by phone online you can ask for an appeal yourself. Web follow the simple instructions below: This form is intended solely for pcp requesting termination of a. Contact us, or refer to the number on the. 4205 philips farm road, suite 100.

WELLCARE HEALTH PLANS, INC. FORM 8K EX99.2 PRESENTATION DATED
Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health. You can call wellcare of north. Disputes, reconsiderations and grievances appointment of representative Licensed sales agents available to help you find a plan in missouri A verbal or written expression of dissatisfaction or dispute with health plan policy, procedure, claims.
Wellcare, Medicare Pharmacy Appeals, P.o.
Web member appeal form complete and mail or fax to: Web the member must sign, date, and complete a representative form. This form is intended solely for pcp requesting termination of a. Licensed sales agents available to help you find a plan in missouri
We Have Redesigned Our Website.
A fast appeal is called an expedited reconsideration (part c) or an expedited redetermination (part d). You may also ask a friend, a family member, your provider or a lawyer to help you. Web access key forms for authorizations, claims, pharmacy and more. Web because we, wellcare, denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for redetermination (appeal) of our.
Web Missouri Care Health Plan.
Web medication appeal request form you can use this form to request an appeal when a medication coverage determination request has been denied. Web if your health requires it, ask us to give you a fast appeal. You can call wellcare of north. Web a repository of medicare forms and documents for wellcare providers, covering topics such as authorizations, claims and behavioral health.
Web A Repository Of Medicare Forms And Documents For Wellcare Providers, Covering Topics Such As Authorizations, Claims And Behavioral Health.
Disputes, reconsiderations and grievances appointment of representative Web wellcare by allwell requires a copy of the completed and signed appointment of representative form to process an appeal filed by the member’s representative. Member/subscriber id, provider id, patient name and date of birth, medicare. The person acting on behalf of the member must sign, date and complete the same form.