Superior Vision Authorization Request Form
Superior Vision Authorization Request Form - Web effective may 1, 2021, ear, nose and throat (ent) surgeries, sleep study management and cardiac surgeries need to be verified by turning point. Box 967 rancho cordova, ca 95741. Please contact superior vision regarding your participation status. Edit your superior vision claim form online. Web superior vision services hipaa privacy authorization form please print hereby authorize the use and/or disclosure of my individually identifiable health information as. Web all request forms must continue to be accompanied by the medical record(s) to support the request. Second, see your eye care professional and pay for your. Web send superior vision authorization form via email, link, or fax. Type signnow.com in your phone’s web browser and sign in to your profile. Please retain the original for your records.
Web superior vision contracts with various lasik networks. Type signnow.com in your phone’s web browser and sign in to your profile. Web send superior vision authorization form via email, link, or fax. To proceed with learning about available. Edit your superior vision claim form online. Web superior vision is a product offering from versant health, a company forged from the experience of two leading vision care plans. Second, see your eye care professional and pay for your. Please retain the original for your records. Web effective may 1, 2021, ear, nose and throat (ent) surgeries, sleep study management and cardiac surgeries need to be verified by turning point. Web this form to the contact information below.
You may electronically submit claims via the company’s website. Web the provider’s choice of optical laboratory does not affect coverage determinations and reimbursements. Web superior vision is a product offering from versant health, a company forged from the experience of two leading vision care plans. Web just log in with your id to get started. Web this form to the contact information below. Web all request forms must continue to be accompanied by the medical record(s) to support the request. You can reach superior vision’s provider relations. Web send superior vision authorization form via email, link, or fax. Web routine vision services authorization request form return fax to: Depending on your benefit coverage, a lasik discount or allowance may be included.
FREE 13+ Prior Authorization Forms in PDF MS Word
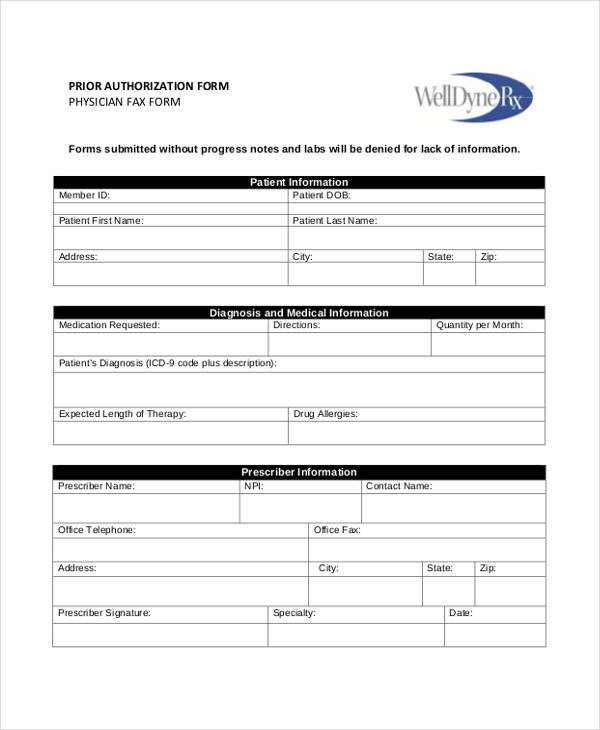
Please retain the original for your records. Web just log in with your id to get started. Web superior vision services hipaa privacy authorization form please print hereby authorize the use and/or disclosure of my individually identifiable health information as. Web send superior vision authorization form via email, link, or fax. Web request for prior authorization request for prior authorization.

Covermymeds Prior Authorization Form Pdf Form Resume Examples
Web the provider’s choice of optical laboratory does not affect coverage determinations and reimbursements. Please contact superior vision regarding your participation status. You can also download it, export it or print it out. Second, see your eye care professional and pay for your. Please retain the original for your records.
Free MedImpact Prior (Rx) Authorization Form PDF eForms
Please retain the original for your records. Web all request forms must continue to be accompanied by the medical record(s) to support the request. Web the provider’s choice of optical laboratory does not affect coverage determinations and reimbursements. Web this form to the contact information below. Web routine vision services authorization request form return fax to:
FREE 13+ Prior Authorization Forms in PDF MS Word
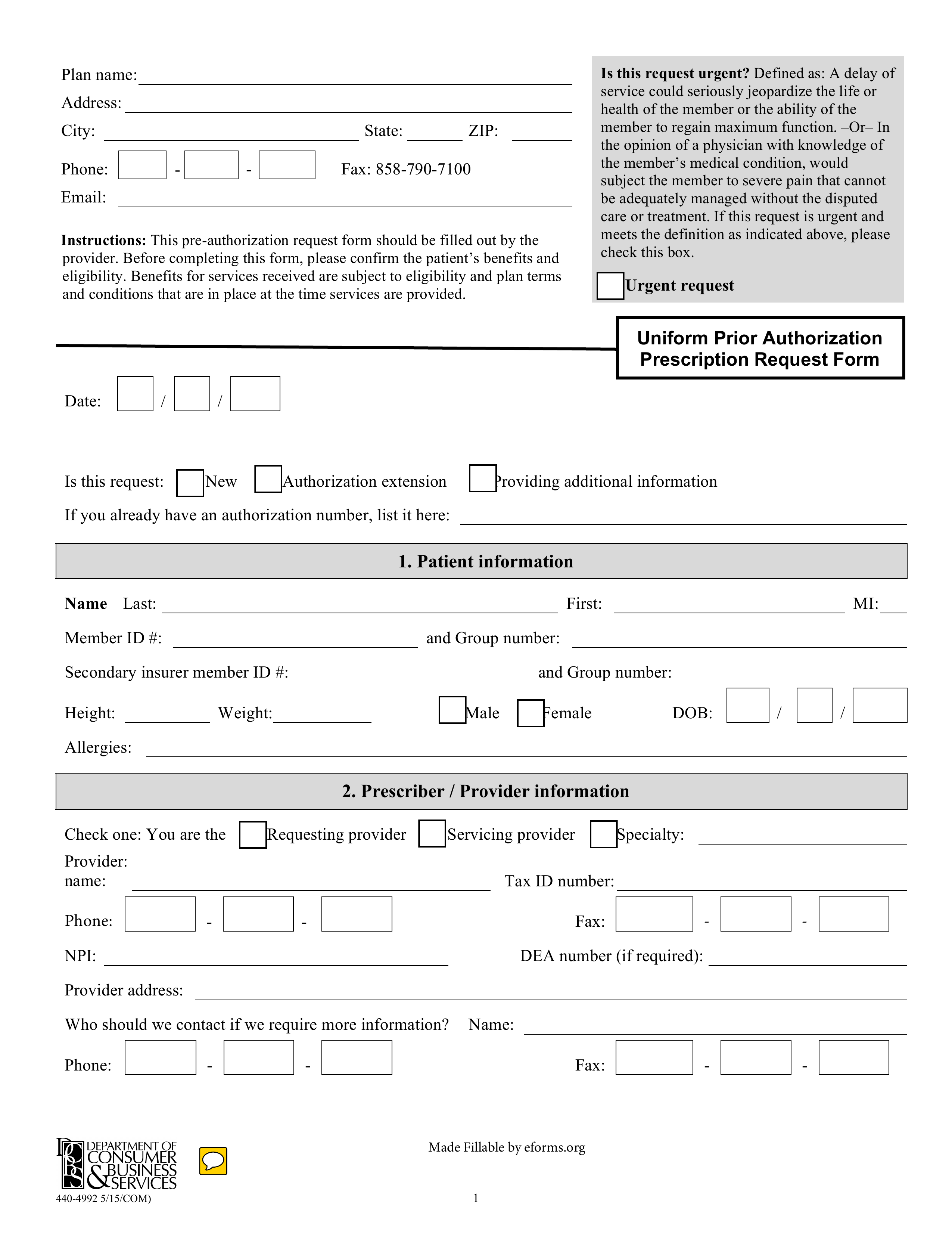
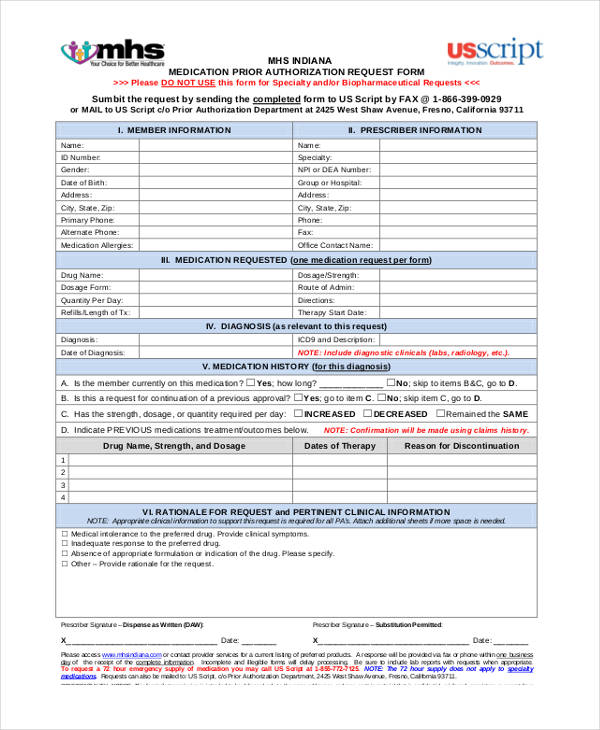
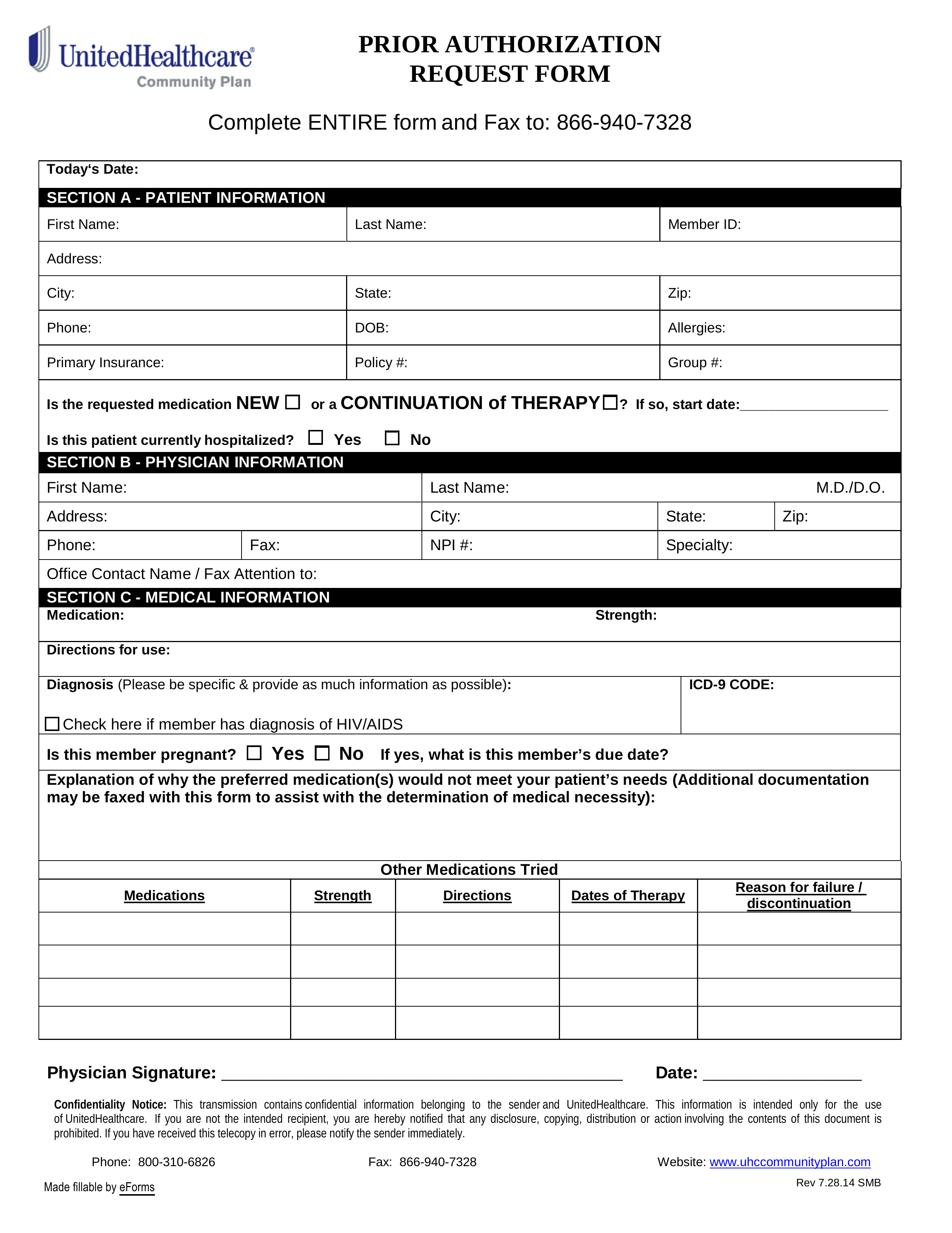
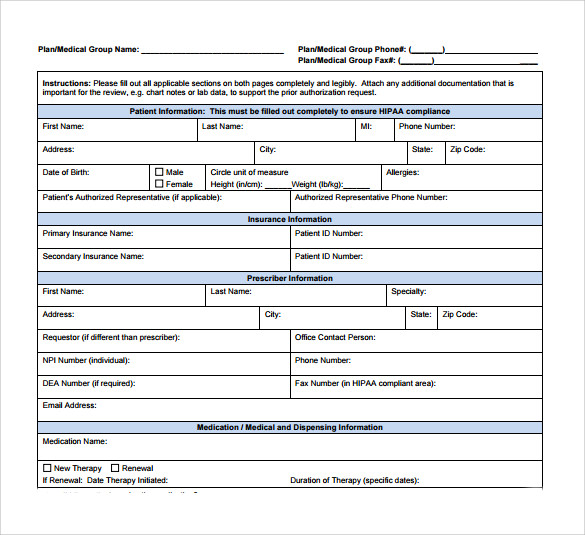
Web providers should include a completed authorization request form and all required documentation and clinical information with an authorization request. You can reach superior vision’s provider relations. Type signnow.com in your phone’s web browser and sign in to your profile. Web effective may 1, 2021, ear, nose and throat (ent) surgeries, sleep study management and cardiac surgeries need to be.
Free UnitedHealthcare Prior (Rx) Authorization Form PDF eForms
For general inquiries, authorizations, and order placement, you can contact us: Web with superior vision, what do i do? Edit your superior vision claim form online. To proceed with learning about available. Web send superior vision authorization form via email, link, or fax.

FREE 11+ Prior Authorization Forms in PDF MS Word
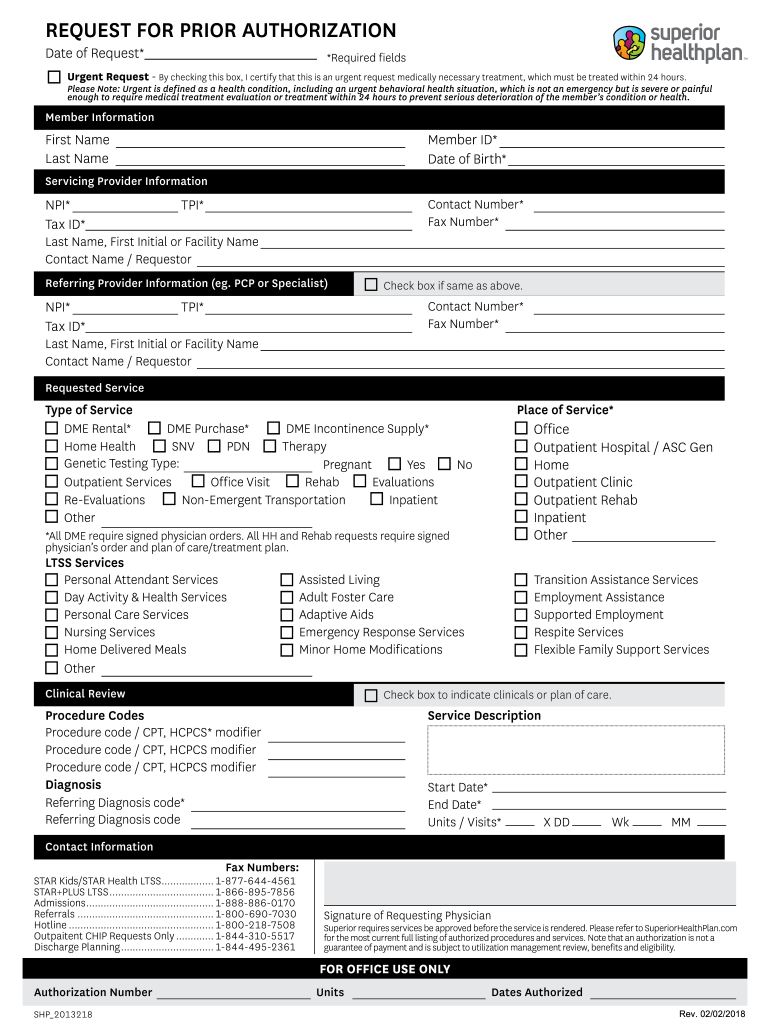
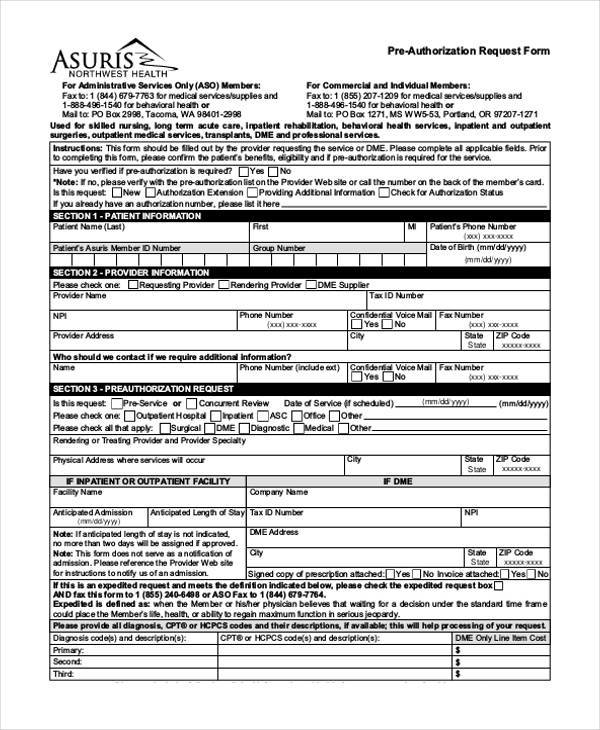
The telephone number to call for notifying superior vision of services. Web request for prior authorization request for prior authorization date of request* *required fields urgent request by checking this box, i certify that. Web this form to the contact information below. Web the provider’s choice of optical laboratory does not affect coverage determinations and reimbursements. Web superior vision services.
FREE 10+ Sample Authorization Request Forms in MS Word PDF
Type signnow.com in your phone’s web browser and sign in to your profile. Web to request prior authorization you can fax or email your request with supporting clinical information regarding the member’s condition to superior vision all prior authorizations. Web request for prior authorization request for prior authorization date of request* *required fields urgent request by checking this box, i.
FREE 8+ Sample Caremark Prior Authorization Forms in PDF
You may electronically submit claims via the company’s website. For general inquiries, authorizations, and order placement, you can contact us: Please contact superior vision regarding your participation status. Web all request forms must continue to be accompanied by the medical record(s) to support the request. Web effective may 1, 2021, ear, nose and throat (ent) surgeries, sleep study management and.
Superior Authorization Form Fill Out and Sign Printable PDF Template
Second, see your eye care professional and pay for your. Web routine vision services authorization request form return fax to: Web request for prior authorization request for prior authorization date of request* *required fields urgent request by checking this box, i certify that. Depending on your benefit coverage, a lasik discount or allowance may be included. Web just log in.
FREE 41+ Authorization Forms in PDF Excel MS word
Depending on your benefit coverage, a lasik discount or allowance may be included. Web with superior vision, what do i do? Please contact superior vision regarding your participation status. Type signnow.com in your phone’s web browser and sign in to your profile. You may electronically submit claims via the company’s website.
Web All Request Forms Must Continue To Be Accompanied By The Medical Record(S) To Support The Request.
Web this form to the contact information below. Web send superior vision authorization form via email, link, or fax. Edit your superior vision claim form online. You can reach superior vision’s provider relations.
Web Just Log In With Your Id To Get Started.
Web providers should include a completed authorization request form and all required documentation and clinical information with an authorization request. To proceed with learning about available. You may electronically submit claims via the company’s website. Web get printable superior vision claim form signed right from your mobile phone using these 6 steps:
Type Signnow.com In Your Phone’s Web Browser And Sign In To Your Profile.
Web effective may 1, 2021, ear, nose and throat (ent) surgeries, sleep study management and cardiac surgeries need to be verified by turning point. Web the provider’s choice of optical laboratory does not affect coverage determinations and reimbursements. Web to request prior authorization you can fax or email your request with supporting clinical information regarding the member’s condition to superior vision all prior authorizations. The telephone number to call for notifying superior vision of services.
Please Retain The Original For Your Records.
Box 967 rancho cordova, ca 95741. Web superior vision services hipaa privacy authorization form please print hereby authorize the use and/or disclosure of my individually identifiable health information as. Web with superior vision, what do i do? You can also download it, export it or print it out.