Provider Inquiry Form Delta Dental
Provider Inquiry Form Delta Dental - Delta dental is comprised of 39 member companies offering dental coverage in all 50 states, puerto rico and other u.s. Deltadentalrequires providers use a resubmission request by selecting that option on this form to resubmit claims for clerical. Can i participate with only one of delta dental's. It is not necessary to call. Web click here for instructions on how to register using your medical provider information. Web please return this form to your local delta dental: Delta dental patient direct coverage are not available in. Cobra continuation of group dental coverage form. Fields marked with an asterisk (*) are required. Use this form to evaluate the conditions that may or may not qualify patients for coverage of.
Web provider refund submission form complete this form when your oce determines an overpayment has been made on one of your patients. Once we receive the completed forms and/or confirmation from the clearinghouse to set. Web download our most used provider forms. Delta dental requires both the eft and era forms to be completed. Territories, with a local presence in. Web online support for delta dental ppo and delta dental premier networks. For inquiries regarding the deltapreferred option usa network, please contact your local delta plan. Web visit a dentist in your network to get the most savings. Can i participate with only one of delta dental's. Search for a network dentist near your home or work.
Web once the registration process is complete you can access delta dental websites with the same username and password. Territories, with a local presence in. Delta dental patient direct coverage are not available in. Begin by logging in with your current username and. Web looking for a dentist? Delta dental of california attn: Web you can determine eligibility for all delta dental members by signing in to your dentist dashboard on deltadental.com. Web please return this form to your local delta dental: Search for a network dentist near your home or work. It is not necessary to call.

Delta Dental Provider Directory Chandler Unified .Delta Dental of
Use this form to evaluate the conditions that may or may not qualify patients for coverage of. For inquiries regarding the deltapreferred option usa network, please contact your local delta plan. Web online support for delta dental ppo and delta dental premier networks. Web community care network (ccn) online dentist inquiry form. Once we receive the completed forms and/or confirmation.
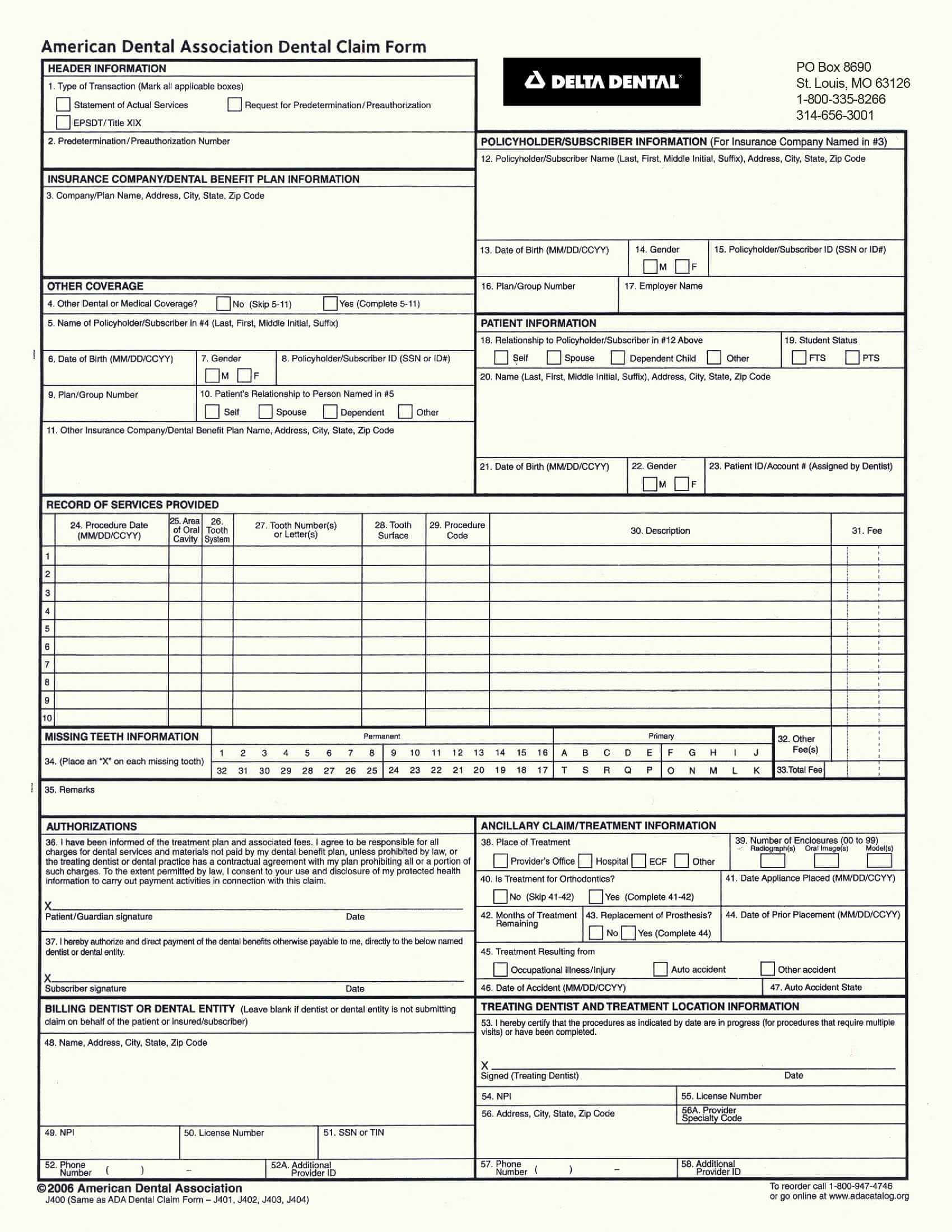
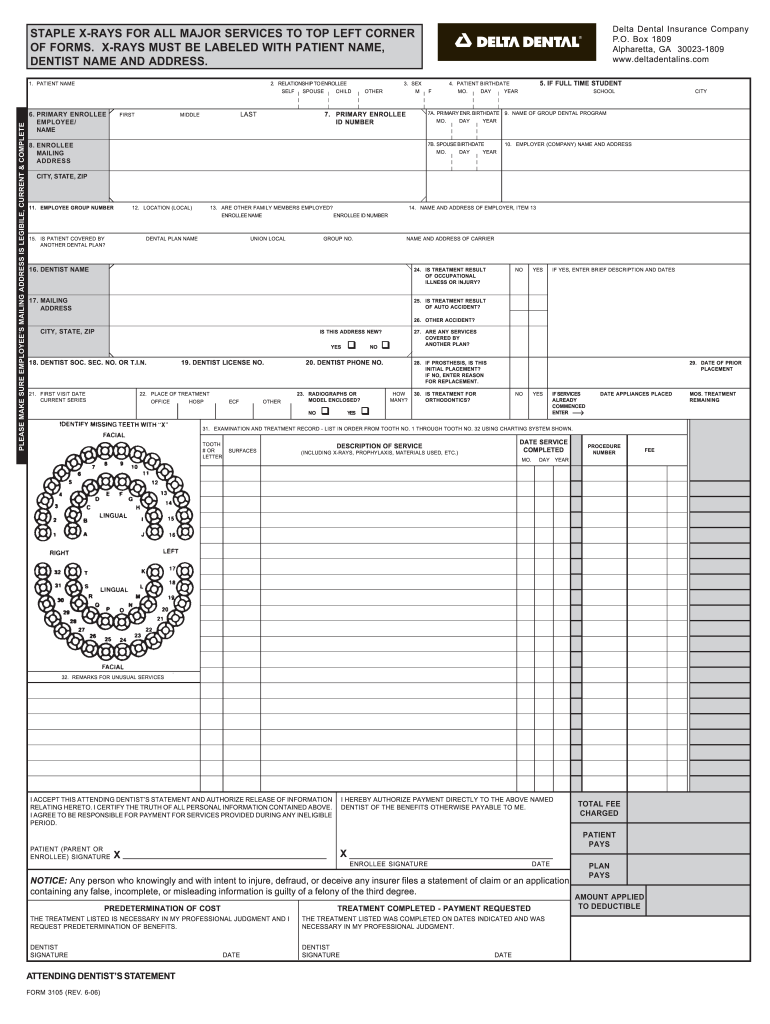
Delta Dental Claim Form
No response may cause processing delays and require. Web you can determine eligibility for all delta dental members by signing in to your dentist dashboard on deltadental.com. As part of our commitment to continually enhance service for our members and your patients, delta dental wants to know more about their dental care. Web click here for instructions on how to.
Top 52 Delta Dental Forms And Templates free to download in PDF format
Web visit a dentist in your network to get the most savings. Delta dental patient direct coverage are not available in. Use this form to evaluate the conditions that may or may not qualify patients for coverage of. Web you can determine eligibility for all delta dental members by signing in to your dentist dashboard on deltadental.com. Cobra continuation of.

Delta Dental Providers Near Me How Do Dental Benefits Work?
Delta dental of california attn: Once we receive the completed forms and/or confirmation from the clearinghouse to set. Begin by logging in with your current username and. Web community care network (ccn) online dentist inquiry form. Deltadentalrequires providers use a resubmission request by selecting that option on this form to resubmit claims for clerical.

Delta Dental Claim Form Fill Online, Printable, Fillable, Blank
Territories, with a local presence in. Web please return this form to your local delta dental: Use this form to evaluate the conditions that may or may not qualify patients for coverage of. I tried using the dental office toolkit for eligibility,. Web instructions read all instructions carefully prior to submitting your application.

IA Wellmark BCBS P4602 20202021 Fill and Sign Printable Template
Deltadentalrequires providers use a resubmission request by selecting that option on this form to resubmit claims for clerical. Web please return this form to your local delta dental: Can i participate with only one of delta dental's. Use this form for standard dental claims. Web online support for delta dental ppo and delta dental premier networks.
Delta Dental Tax Form Fill Out and Sign Printable PDF Template signNow
Can i participate with only one of delta dental's. Web community care network (ccn) online dentist inquiry form. Fields marked with an asterisk (*) are required. Web visit a dentist in your network to get the most savings. Delta dental ppo provider tools overview.
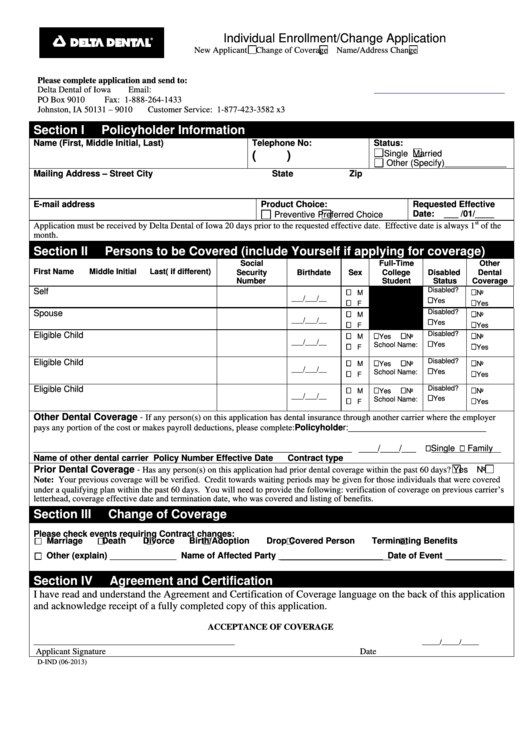
Form DInd Delta Dental Iowa Individual Enrollment Change Application
Deltadentalrequires providers use a resubmission request by selecting that option on this form to resubmit claims for clerical. As part of our commitment to continually enhance service for our members and your patients, delta dental wants to know more about their dental care. Can i participate with only one of delta dental's. Use this form to evaluate the conditions that.
Fillable Provider Inquiry Process Paper Provider Inquiry Form
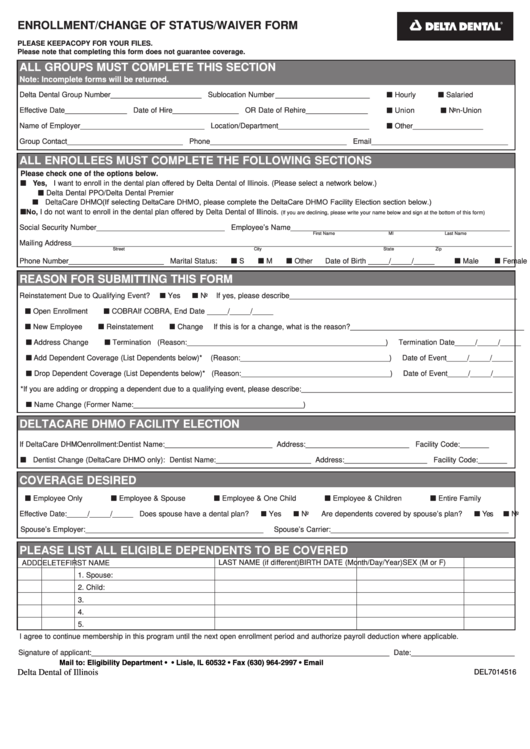
As part of our commitment to continually enhance service for our members and your patients, delta dental wants to know more about their dental care. Authorization for disclosure of protected health information. Cobra continuation of group dental coverage form. For inquiries regarding the deltapreferred option usa network, please contact your local delta plan. Fields marked with an asterisk (*) are.
Fillable Form Gr69140 Aetna Practitioner And Provider Complaint And
Use this form to evaluate the conditions that may or may not qualify patients for coverage of. Delta dental is comprised of 39 member companies offering dental coverage in all 50 states, puerto rico and other u.s. Use this form for standard dental claims. Once we receive the completed forms and/or confirmation from the clearinghouse to set. Delta dental patient.
Deltadentalrequires Providers Use A Resubmission Request By Selecting That Option On This Form To Resubmit Claims For Clerical.
Web download our most used provider forms. Web click here for instructions on how to register using your medical provider information. Delta dental patient direct coverage are not available in. Begin by logging in with your current username and.
Web Please Return This Form To Your Local Delta Dental:
Delta dental ppo provider tools overview. Web community care network (ccn) online dentist inquiry form. Search for a network dentist near your home or work. Cobra continuation of group dental coverage form.
Fields Marked With An Asterisk (*) Are Required.
Web once the registration process is complete you can access delta dental websites with the same username and password. It is not necessary to call. Use this form for standard dental claims. Web required information to access records regarding your request:
Once We Receive The Completed Forms And/Or Confirmation From The Clearinghouse To Set.
Web online support for delta dental ppo and delta dental premier networks. Web visit a dentist in your network to get the most savings. Web provider refund submission form complete this form when your oce determines an overpayment has been made on one of your patients. As part of our commitment to continually enhance service for our members and your patients, delta dental wants to know more about their dental care.