Physical Therapy Medical History Form
Physical Therapy Medical History Form - Web yes no yes no neck injury/surgery ____ ____ stroke/tia ____ ____ Web physical therapy intake form is a set of questions related to the patient’s personal information, lifestyle, family medical history, nature of work, and past medical history which is very essential to better understand the medical condition of the patient. Web what is your goal for therapy at this time? Breakthrough physical therapy hipaa consent form. Yes no b) do you currently have an infection? Web dull ache sharp stiffness constant worse in a.m. Breakthrough physical therapy general photo/video release form. Web physical therapist other (specify: Therapist comments do you have high blood pressure? Signature of patient or guardian (if patient is a minor):
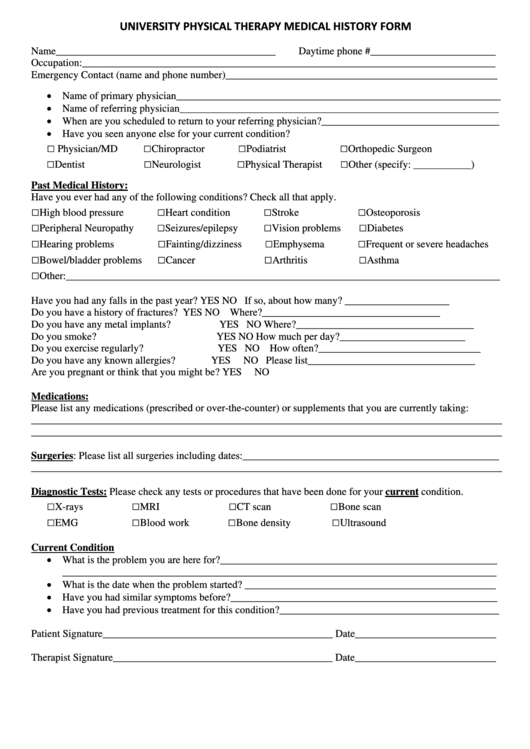
High blood pressure heart condition stroke osteoporosis peripheral neuropathy seizures/epilepsy Have you ever had any of the following conditions? Stair climbing standing other name Web what is your goal for therapy at this time? Web physical therapist other (specify: Web general physical therapy forms. Therapist comments do you have high blood pressure? Web i, the undersigned, do hereby agree and give my consent for progress rehabilitation network, llc, d/b/a integrated sports medicine and physical therapy, llc (“clinic”) to furnish medical care and treatment to, _____, considered necessary and proper in diagnosing or treating his/her physical condition. Signature of patient or guardian (if patient is a minor): Web yes no yes no neck injury/surgery ____ ____ stroke/tia ____ ____
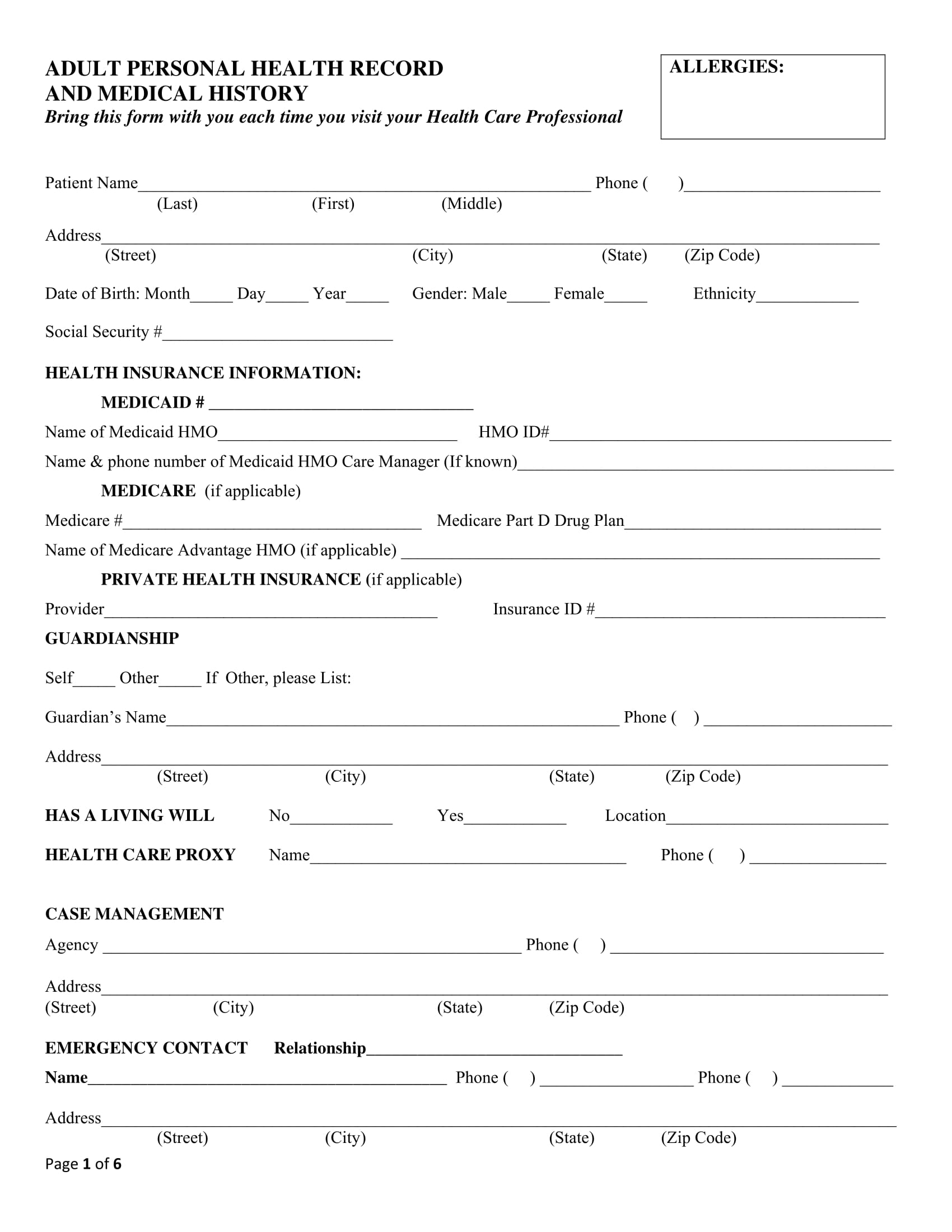
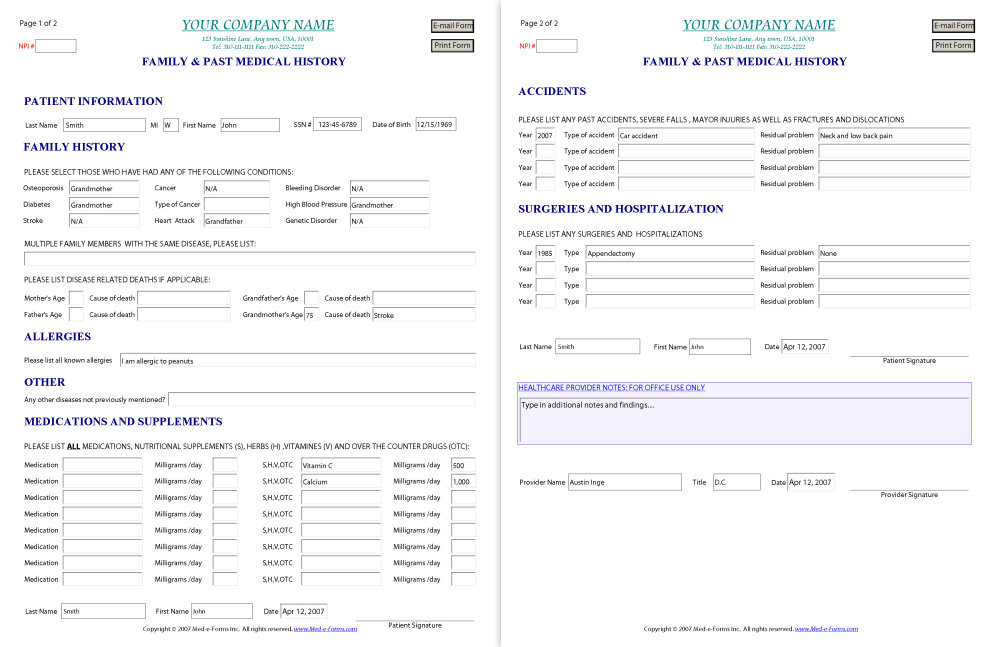
Web physical therapy intake form is a set of questions related to the patient’s personal information, lifestyle, family medical history, nature of work, and past medical history which is very essential to better understand the medical condition of the patient. Web find a clinic request appointment check insurance patient forms. Web physical therapy history intake form referring md: Breakthrough physical therapy hipaa consent form. High blood pressure heart condition stroke osteoporosis peripheral neuropathy seizures/epilepsy Web yes no yes no neck injury/surgery ____ ____ stroke/tia ____ ____ Breakthrough physical therapy general photo/video release form. Breakthrough physical therapy medical history form. Signature of patient or guardian (if patient is a minor): Please circle the appropriate answer:
FREE 6+ Medical History Forms in PDF MS Word Excel
What is your reason for coming to therapy today? Web i, the undersigned, do hereby agree and give my consent for progress rehabilitation network, llc, d/b/a integrated sports medicine and physical therapy, llc (“clinic”) to furnish medical care and treatment to, _____, considered necessary and proper in diagnosing or treating his/her physical condition. Web physical therapy intake form is a.

Alliance Rehab & Physical Therapy Medical History
Have you ever had any of the following conditions? Signature of patient or guardian (if patient is a minor): Web what is your goal for therapy at this time? Breakthrough physical therapy hipaa consent form. Please circle the appropriate answer:
Medical History Form Template templates free printable
Please circle the appropriate answer: What is your reason for coming to therapy today? Complete the forms at your convenience, and remember to bring them with you to your first scheduled visit. Web physical therapy intake form is a set of questions related to the patient’s personal information, lifestyle, family medical history, nature of work, and past medical history which.
University Physical Therapy Medical History Form printable pdf download
Breakthrough physical therapy hipaa consent form. Please circle the appropriate answer: In preparation for your first appointment with professional physical therapy, please print the patient forms below. Have you ever had any of the following conditions? How did your problem start?
Medical History Form 9+ Free PDF Documents Download
What is your reason for coming to therapy today? Breakthrough physical therapy hipaa consent form. Web physical therapy history intake form referring md: Therapist comments do you have high blood pressure? Complete the forms at your convenience, and remember to bring them with you to your first scheduled visit.

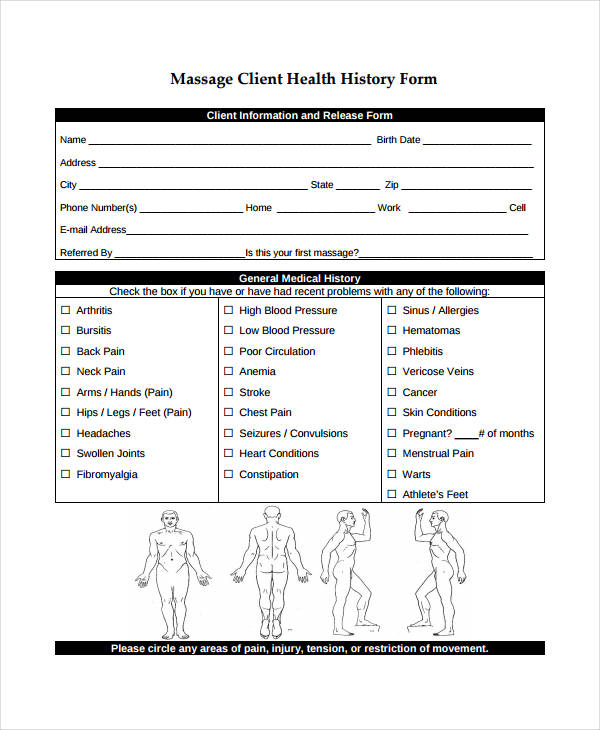
massage therapy consent forms free Google Search massage massage
Breakthrough physical therapy patient information form. Web what is your goal for therapy at this time? Therapist comments do you have high blood pressure? What is your reason for coming to therapy today? High blood pressure heart condition stroke osteoporosis peripheral neuropathy seizures/epilepsy
Medical History Forms
Breakthrough physical therapy general photo/video release form. Breakthrough physical therapy medical history form. When did your problem begin? High blood pressure heart condition stroke osteoporosis peripheral neuropathy seizures/epilepsy Breakthrough physical therapy patient communication preferences.
FREE 12+ Sample Medical History Forms in PDF MS Word Excel
Web physical therapy intake form is a set of questions related to the patient’s personal information, lifestyle, family medical history, nature of work, and past medical history which is very essential to better understand the medical condition of the patient. High blood pressure heart condition stroke osteoporosis peripheral neuropathy seizures/epilepsy Web dull ache sharp stiffness constant worse in a.m. In.
Patient Medical History Form Fill Out and Sign Printable PDF Template
Web yes no yes no neck injury/surgery ____ ____ stroke/tia ____ ____ How did your problem start? Breakthrough physical therapy patient communication preferences. Therapist comments do you have high blood pressure? Web physical therapy history intake form referring md:

28 Acupuncture Intake form Template in 2020 Massage intake forms
Web find a clinic request appointment check insurance patient forms. Stair climbing standing other name Breakthrough physical therapy medical history form. High blood pressure heart condition stroke osteoporosis peripheral neuropathy seizures/epilepsy Web general physical therapy forms.
Therapist Comments Do You Have High Blood Pressure?
Breakthrough physical therapy patient communication preferences. Breakthrough physical therapy medical history form. Web physical therapy intake form is a set of questions related to the patient’s personal information, lifestyle, family medical history, nature of work, and past medical history which is very essential to better understand the medical condition of the patient. Web physical therapy history intake form referring md:
When Did Your Problem Begin?
High blood pressure heart condition stroke osteoporosis peripheral neuropathy seizures/epilepsy Breakthrough physical therapy patient information form. Signature of patient or guardian (if patient is a minor): Stair climbing standing other name
Web Physical Therapist Other (Specify:
Web dull ache sharp stiffness constant worse in a.m. Web yes no yes no neck injury/surgery ____ ____ stroke/tia ____ ____ Web general physical therapy forms. Breakthrough physical therapy hipaa consent form.
Breakthrough Physical Therapy General Photo/Video Release Form.
Web i, the undersigned, do hereby agree and give my consent for progress rehabilitation network, llc, d/b/a integrated sports medicine and physical therapy, llc (“clinic”) to furnish medical care and treatment to, _____, considered necessary and proper in diagnosing or treating his/her physical condition. Yes no b) do you currently have an infection? Complete the forms at your convenience, and remember to bring them with you to your first scheduled visit. In preparation for your first appointment with professional physical therapy, please print the patient forms below.