Phi Release Form
Phi Release Form - The information solicited on this form will be used to provide all paper and electronic medical records as requested. To for the purpose of (provide a detailed description): Web to request a change, fill out the upmc patient amendment to phi form. Completed by date mrn release id authr 18534 (2/2023) state zip code phone number street address previous last name (if any) city patient name date of birth patient information purpose for release. The information on this form may be shared with the requester or person authorized by the requester. Web direct access to pdf of hipaa release. Name of doctor/hospital/insurance company/other agency, person, or self: Web by writing to the address on this form. • whoever gets my phi may share it with others. Each section needs to be completed to be valid.
Name of doctor/hospital/insurance company/other agency, person, or self: The process may take up to 60 days. To for the purpose of (provide a detailed description): Upmc can also deny the request if we deem your record correct and complete. Hereby consent to and authorize the above entities to release information from my medical record to: Web to request a change, fill out the upmc patient amendment to phi form. • whoever gets my phi may share it with others. Web patient authorization for release of protected health information internal use only instructions for completing and mailing this form are on page 2. Web by writing to the address on this form. Free immediate download of pdf.
Parts 1 and 2 must be completed to properly identify the records to be released. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family member or friend) such as an insurance company, employer, or for legal purposes, etc. Type of records to be released and approximate date(s) of service (check all. Web authorization for release of protected health information i authorize to release information from the record of: • my chance to sign up for insurance will not change if i don’t sign this form. Upmc can also deny the request if we deem your record correct and complete. To for the purpose of (provide a detailed description): Web by writing to the address on this form. It is a hipaa violation to release medical records without a hipaa authorization form. The process may take up to 60 days.
FREE 23+ Patient Release Forms in PDF MS Word
Web direct access to pdf of hipaa release. The information on this form may be shared with the requester or person authorized by the requester. It won’t take back the phi we already shared. Each section needs to be completed to be valid. Free immediate download of pdf.
Fillable Authorization For Release Of Protected Health Information (Phi
The information solicited on this form will be used to provide all paper and electronic medical records as requested. It won’t take back the phi we already shared. Please note, we may consult your doctor before making changes to your record. Name of doctor/hospital/insurance company/other agency, person, or self: Web by writing to the address on this form.
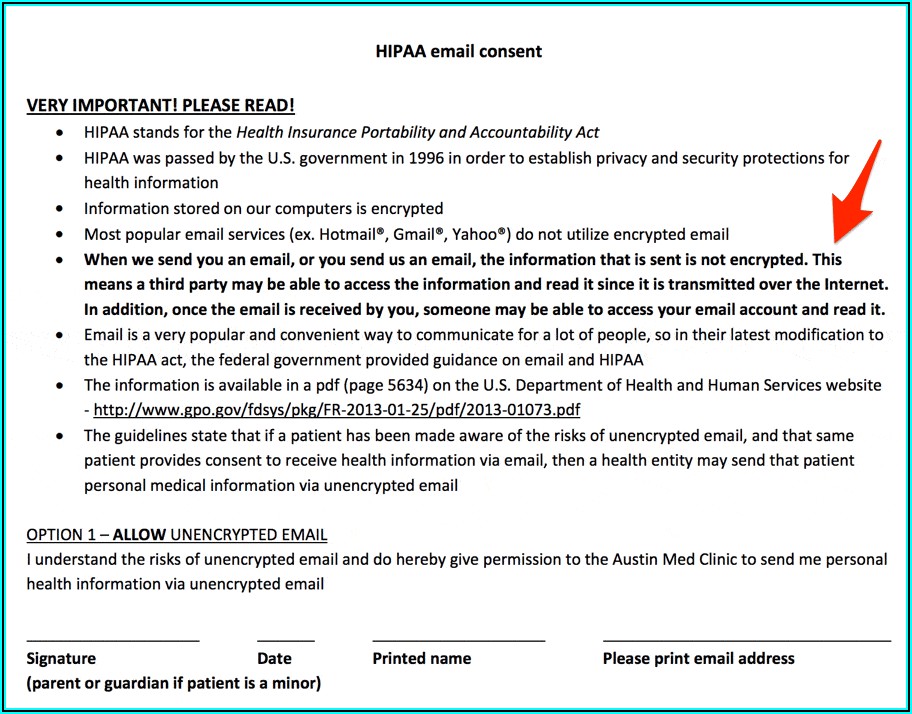
Hipaa Sample Form Form Resume Examples QJ9eJlZYmy
Web patient authorization for release of protected health information internal use only instructions for completing and mailing this form are on page 2. • whoever gets my phi may share it with others. • if you take back your. To for the purpose of (provide a detailed description): It won’t take back the phi we already shared.
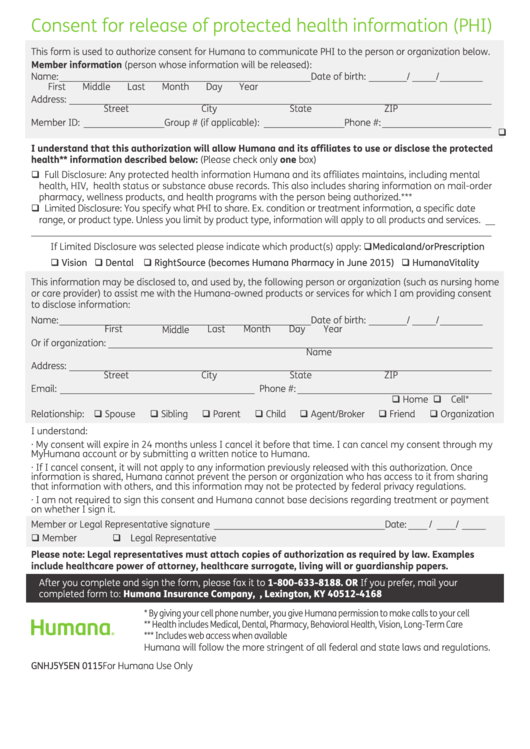
Fillable Consent For Release Of Protected Health Information (Phi) Form
It won’t take back the phi we already shared. Upmc can also deny the request if we deem your record correct and complete. • if you take back your. Web patient authorization for release of protected health information internal use only instructions for completing and mailing this form are on page 2. That means laws may not be able to.
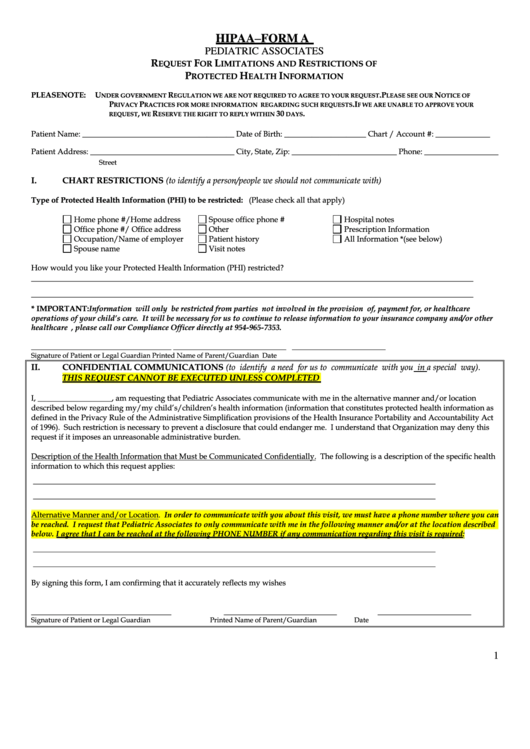
Hipaa Form A Request For Limitations And Restrictions Of Protected
Its purpose is to protect and safeguard protected health information (phi) when. The process may take up to 60 days. Completed by date mrn release id authr 18534 (2/2023) state zip code phone number street address previous last name (if any) city patient name date of birth patient information purpose for release. The information solicited on this form will be.

Oklahoma Authorization Health Fill Online, Printable, Fillable, Blank
Free immediate download of pdf. Web direct access to pdf of hipaa release. Please note, we may consult your doctor before making changes to your record. The process may take up to 60 days. This form is to be used by a patient or legal representative to authorize the release of information to a third party (other than a family.
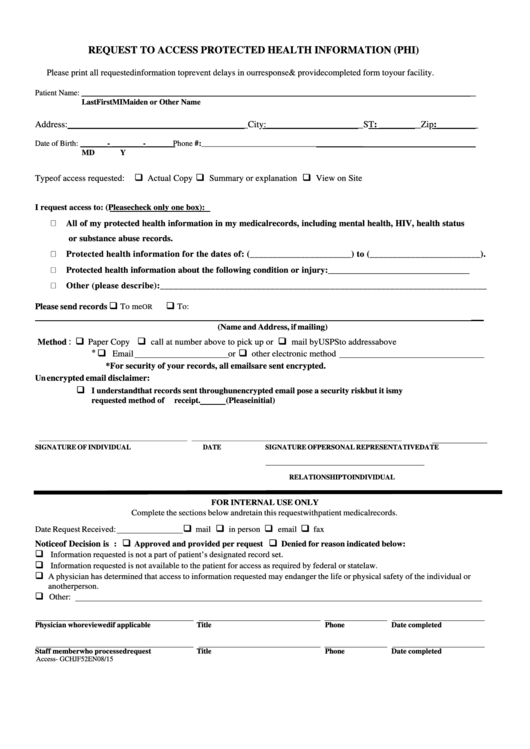
Request To Access Protected Health Information (Phi) Form printable pdf
It won’t take back the phi we already shared. Hereby consent to and authorize the above entities to release information from my medical record to: Web authorization for release of protected health information i authorize to release information from the record of: Web patient authorization for release of protected health information internal use only instructions for completing and mailing this.

Form AW18 Download Printable PDF or Fill Online Release of Protected
• my chance to sign up for insurance will not change if i don’t sign this form. Name of doctor/hospital/insurance company/other agency, person, or self: Web patient authorization for release of protected health information internal use only instructions for completing and mailing this form are on page 2. This form is to be used by a patient or legal representative.

Pin on Examples Online Form Templates
Web updated july 17, 2023 hipaa forms are used in accordance with the health insurance portability and accountability act (hipaa) of 1996. Upmc can also deny the request if we deem your record correct and complete. It is a hipaa violation to release medical records without a hipaa authorization form. • my chance to sign up for insurance will not.

Download Missouri Medical Record Release Form for Free FormTemplate
It won’t take back the phi we already shared. Upmc can also deny the request if we deem your record correct and complete. The information on this form may be shared with the requester or person authorized by the requester. But we will not share any more of your phi. To for the purpose of (provide a detailed description):
Completed By Date Mrn Release Id Authr 18534 (2/2023) State Zip Code Phone Number Street Address Previous Last Name (If Any) City Patient Name Date Of Birth Patient Information Purpose For Release.
Web patient authorization for release of protected health information internal use only instructions for completing and mailing this form are on page 2. Hereby consent to and authorize the above entities to release information from my medical record to: Web direct access to pdf of hipaa release. That means laws may not be able to protect my phi.
Upmc Can Also Deny The Request If We Deem Your Record Correct And Complete.
Web to request a change, fill out the upmc patient amendment to phi form. The information solicited on this form will be used to provide all paper and electronic medical records as requested. Web updated july 17, 2023 hipaa forms are used in accordance with the health insurance portability and accountability act (hipaa) of 1996. Parts 1 and 2 must be completed to properly identify the records to be released.
It Won’t Take Back The Phi We Already Shared.
The process may take up to 60 days. Web by writing to the address on this form. Please note, we may consult your doctor before making changes to your record. The information on this form may be shared with the requester or person authorized by the requester.
Name Of Doctor/Hospital/Insurance Company/Other Agency, Person, Or Self:
Then mail it to the proper medical records department. To for the purpose of (provide a detailed description): Free immediate download of pdf. • my chance to sign up for insurance will not change if i don’t sign this form.