Medicare Form Cms 1763
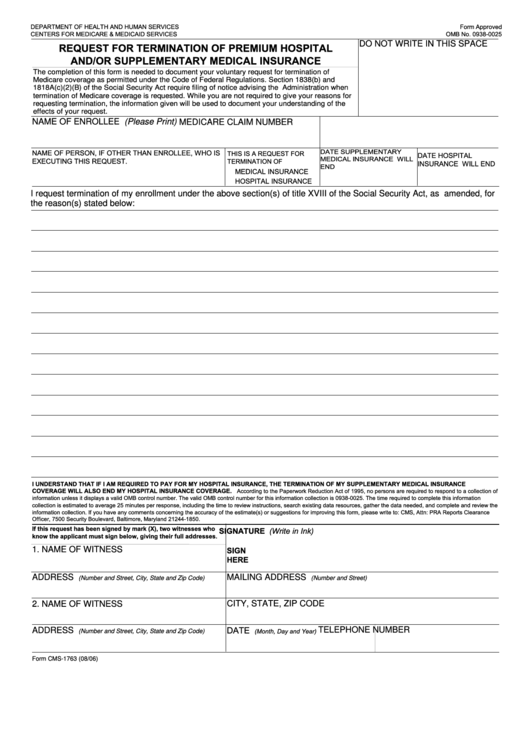
Medicare Form Cms 1763 - Department of health and human services. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted. Request for termination of premium hospital insurance of supplementary medical insurance: National provider identifier (npi) application/update form. Web centers for medicare & medicaid services. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. 05/21) request for termination of premium hospital and/or supplementary medical insurance. Use fill to complete blank online medicare & medicaid pdf forms for free. Hard copy forms may be available from intermediaries, carriers, state agencies, local social security offices or end stage. Many cms program related forms are available in portable document format (pdf).
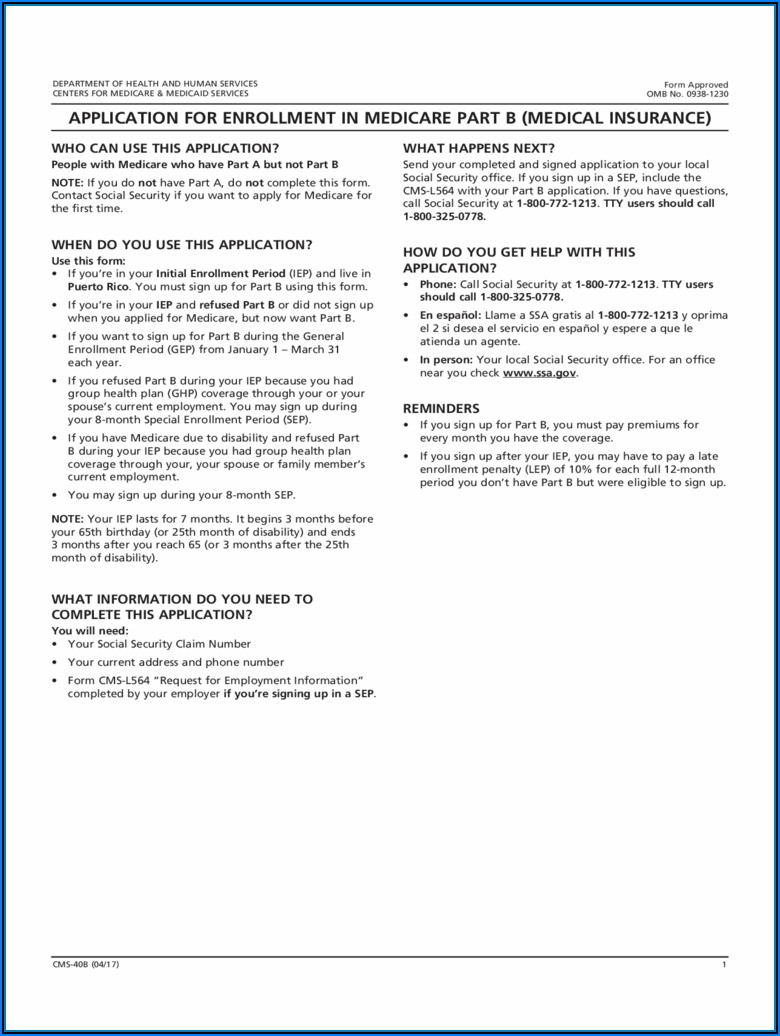
Who can use this form? Use fill to complete blank online medicare & medicaid pdf forms for free. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. People with medicare premium part a or b who would. 05/21) request for termination of premium hospital and/or supplementary medical insurance. National provider identifier (npi) application/update form. Many cms program related forms are available in portable document format (pdf). Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Once completed you can sign your fillable form or send for signing. All forms are printable and downloadable.
People with medicare premium part a or b who would. Request for termination of premium hospital insurance of supplementary medical insurance: Use fill to complete blank online medicare & medicaid pdf forms for free. Once completed you can sign your fillable form or send for signing. Many cms program related forms are available in portable document format (pdf). Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. 05/21) request for termination of premium hospital and/or supplementary medical insurance. Who can use this form? Department of health and human services. Hard copy forms may be available from intermediaries, carriers, state agencies, local social security offices or end stage.
Fillable Request For Termination Of Premium Hospital And/or
Web centers for medicare & medicaid services. Department of health and human services. National provider identifier (npi) application/update form. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted.

Fill Medicare & Medicaid
Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted. Hard copy forms may be available from intermediaries, carriers, state agencies, local social security offices or end stage. Many cms program related forms are available in.
Medicare Part B Form Cms 1763 Form Resume Examples X42M4aXaVk
Web centers for medicare & medicaid services. 05/21) request for termination of premium hospital and/or supplementary medical insurance. Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s. Hard copy forms may be available from intermediaries, carriers, state agencies, local social security offices or end stage. You must submit this form to the social.

Fill Medicare & Medicaid
Many cms program related forms are available in portable document format (pdf). The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted. People with medicare premium part a or b who would. You must submit this form to the social security administration or you may contact them at 1. Hard copy.

CMS 1763 Form Termination of Medical Insurance pdfFiller Blog
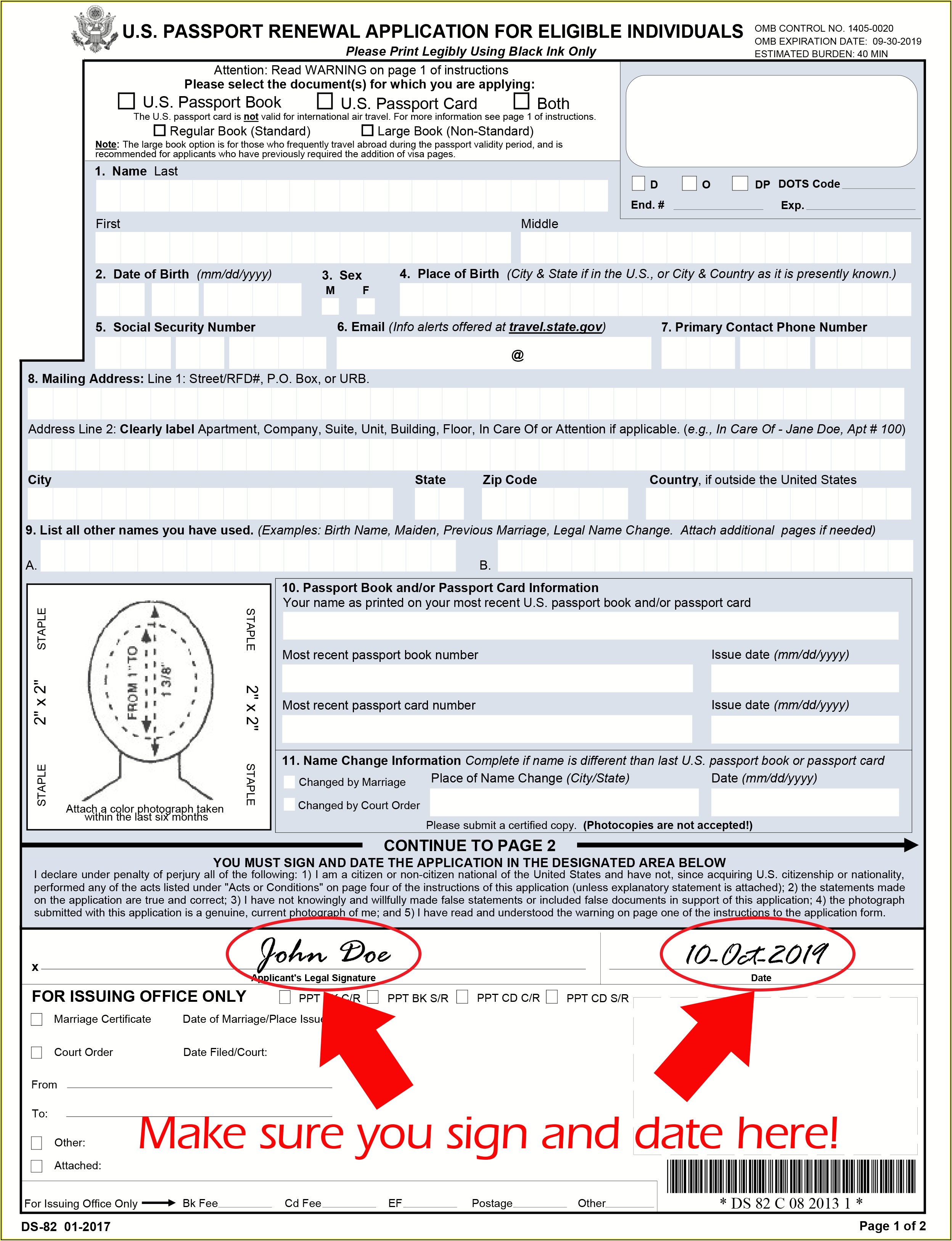
Once completed you can sign your fillable form or send for signing. All forms are printable and downloadable. You must submit this form to the social security administration or you may contact them at 1. People with medicare premium part a or b who would. National provider identifier (npi) application/update form.
Viagra Cost At Optumrx CALL US 3128648200
Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. National provider identifier (npi) application/update form. Many cms program related forms are available in portable document format (pdf). Request for termination of premium hospital insurance of supplementary medical insurance: Web the centers for medicare & medicaid services (cms) is a federal agency within the u.s.
Where Do I Mail Medicare Form Cms 1763 Form Resume Examples AjYdXvKoYl
You must submit this form to the social security administration or you may contact them at 1. Department of health and human services. Once completed you can sign your fillable form or send for signing. Request for termination of premium hospital insurance of supplementary medical insurance: All forms are printable and downloadable.

CMS 1763 How to opt out of your medicare insurance
Department of health and human services. Many cms program related forms are available in portable document format (pdf). All forms are printable and downloadable. You must submit this form to the social security administration or you may contact them at 1. Once completed you can sign your fillable form or send for signing.
Medicare Form Cms 5510 Form Resume Examples Wk9yjr1Y3D
Once completed you can sign your fillable form or send for signing. Use fill to complete blank online medicare & medicaid pdf forms for free. All forms are printable and downloadable. You must submit this form to the social security administration or you may contact them at 1. Hard copy forms may be available from intermediaries, carriers, state agencies, local.
Form CMS1763 Download Fillable PDF or Fill Online Request for
National provider identifier (npi) application/update form. Web centers for medicare & medicaid services. Hard copy forms may be available from intermediaries, carriers, state agencies, local social security offices or end stage. Many cms program related forms are available in portable document format (pdf). People with medicare premium part a or b who would.
Request For Termination Of Premium Hospital Insurance Of Supplementary Medical Insurance:
Who can use this form? You must submit this form to the social security administration or you may contact them at 1. National provider identifier (npi) application/update form. Department of health and human services.
Request For Termination Of Premium Part A, Part B, Or Part B Immunosuppressive Drug Coverage.
All forms are printable and downloadable. Once completed you can sign your fillable form or send for signing. Use fill to complete blank online medicare & medicaid pdf forms for free. 05/21) request for termination of premium hospital and/or supplementary medical insurance.
Web The Centers For Medicare & Medicaid Services (Cms) Is A Federal Agency Within The U.s.
Many cms program related forms are available in portable document format (pdf). The completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted. Web centers for medicare & medicaid services. People with medicare premium part a or b who would.