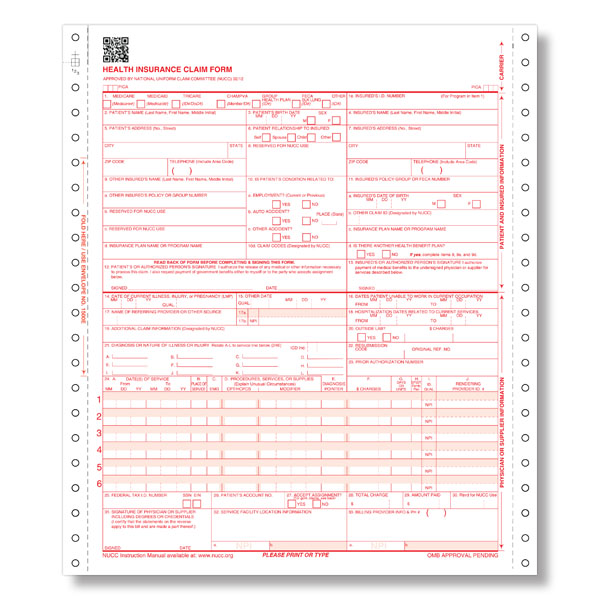
Medical Claim Form 1500
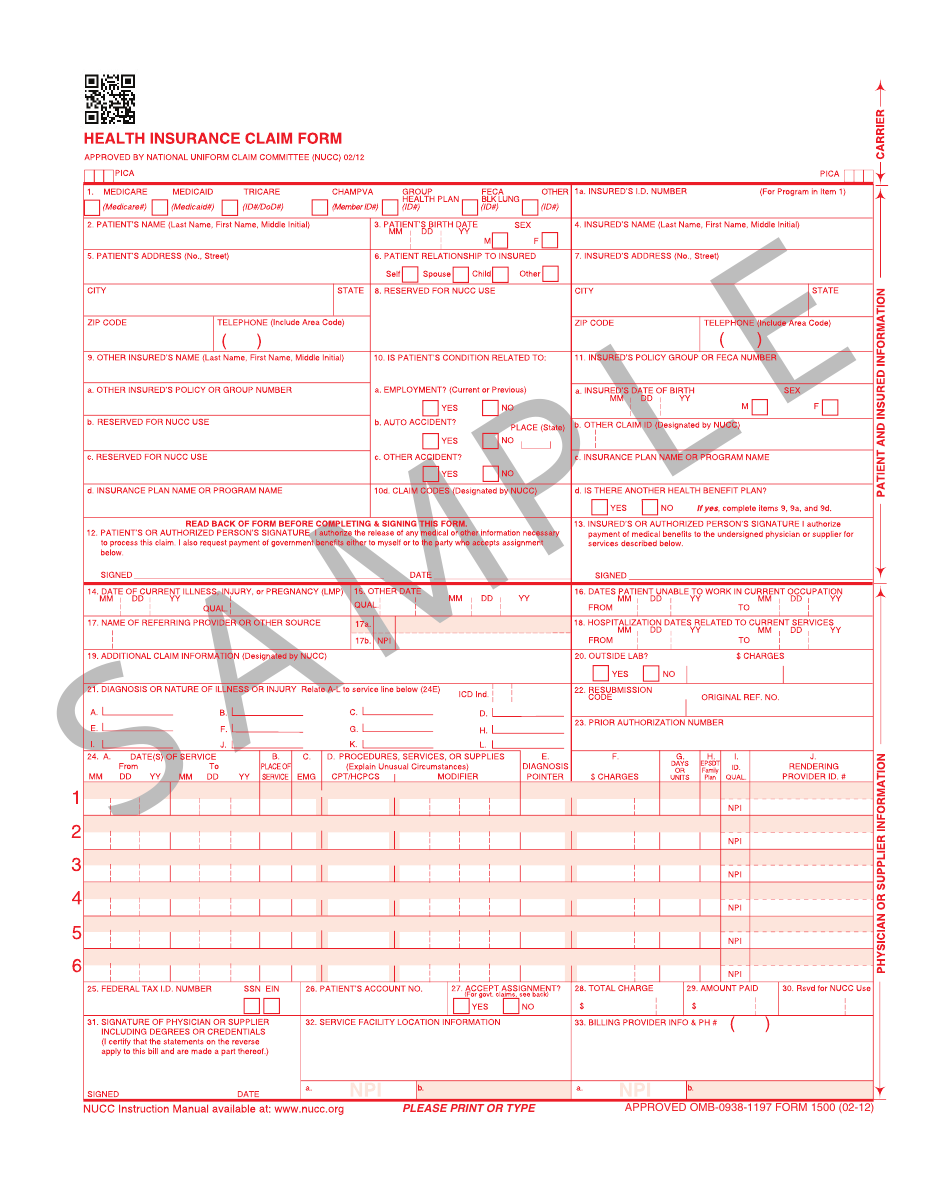
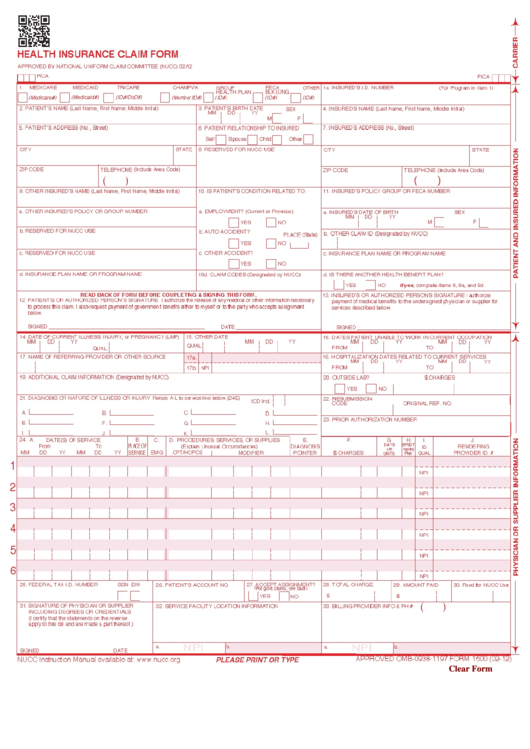
Medical Claim Form 1500 - The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Failure to furnish any other information, such as name or claim number, would delay payment of the claim. Please print or type form hcfa. Web cms 1500 dynamic list information. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Billing info > billing preferences > insurance. You can decide how often to. Medicare medicaid tricare champva other read back of form before completing & signing this form. Health insurance claim form 1.
Web cms 1500 dynamic list information. Download free cms 1500 claim form fillable template. Web health insurance claim form 1. Get everything done in minutes. Number (for program in item 1) 4. Web however, failure to furnish information regarding the medical services rendered or the amount charged would prevent payment of claims under these programs. Read the instructions and tips below first. Insured’s name (last name, first name, middle initial). Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Billing info > billing preferences > insurance.
Billing info > billing preferences > insurance. Read the instructions and tips below first. Failure to provide medical information under feca could be deemed an obstruction. You can decide how often to. Medicare medicaid tricare champva other read back of form before completing & signing this form. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Please print or type form hcfa. Web cms 1500 dynamic list information. Medicare medicaid champus champva other read back of form before completing & signing this form. Web however, failure to furnish information regarding the medical services rendered or the amount charged would prevent payment of claims under these programs.
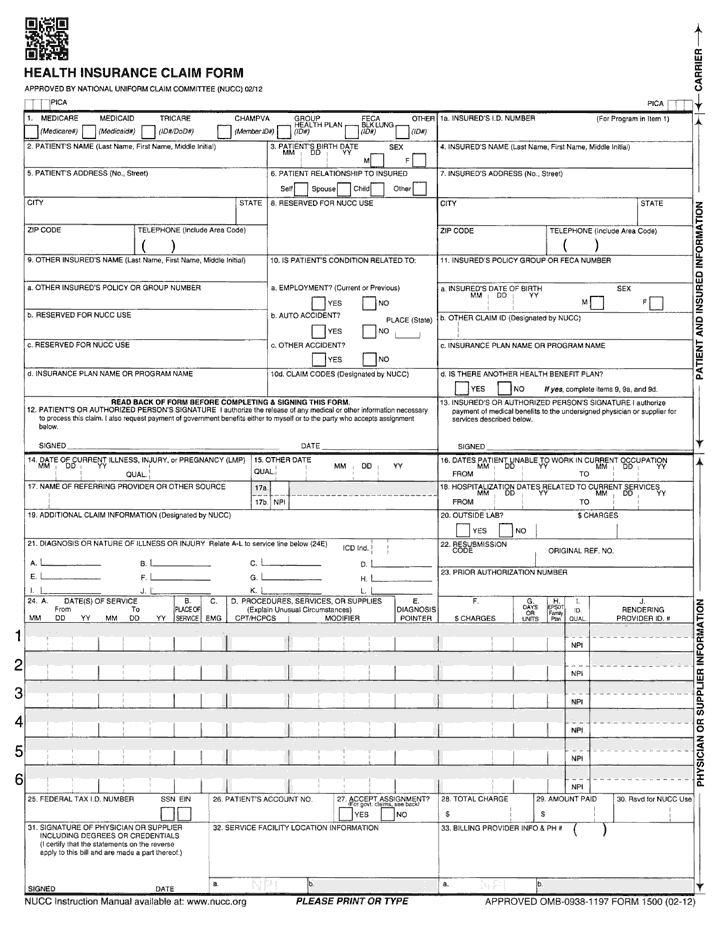
Form 1500 Download Printable PDF or Fill Online Health Insurance Claim
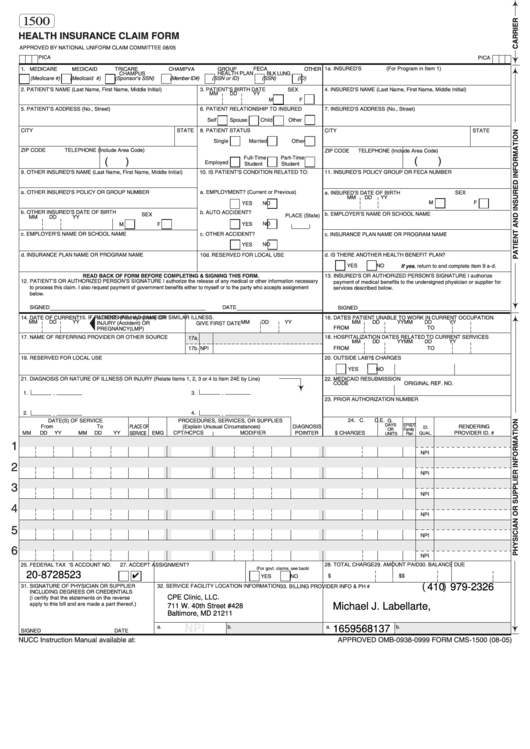
Web health insurance claim form 1. Sign up to get the latest information about your choice of cms topics. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Download free.
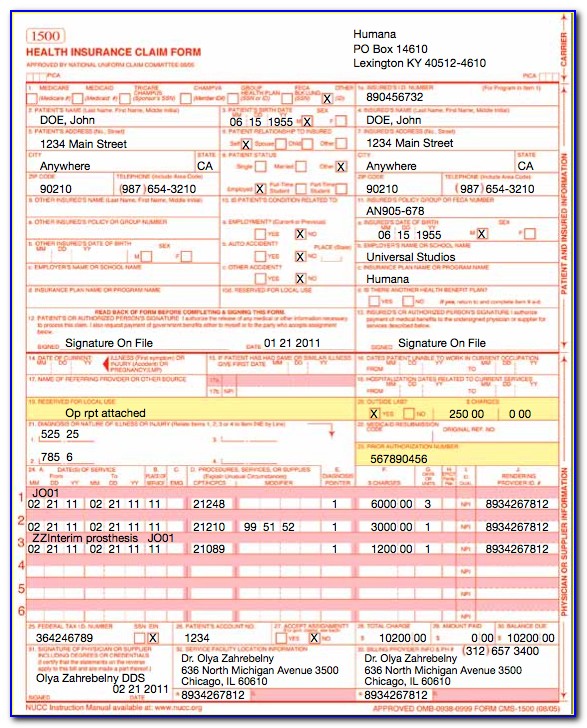
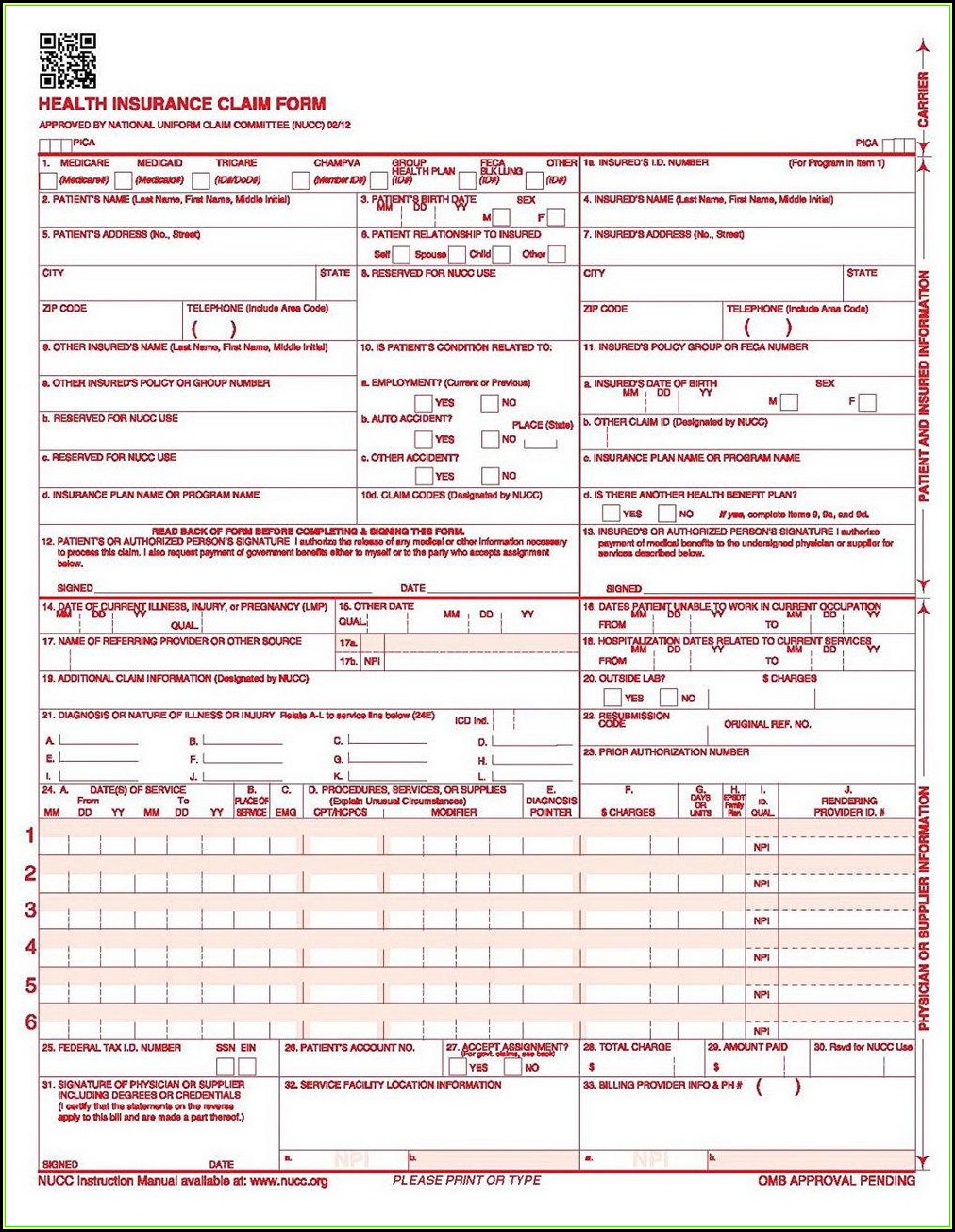
Fillable Form 1500 2005 Health Insurance Claim Form printable pdf
Failure to provide medical information under feca could be deemed an obstruction. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web cms 1500 dynamic list information. Billing info > billing preferences > insurance. The current version of the original manual from the national uniform claim comettee of how to.
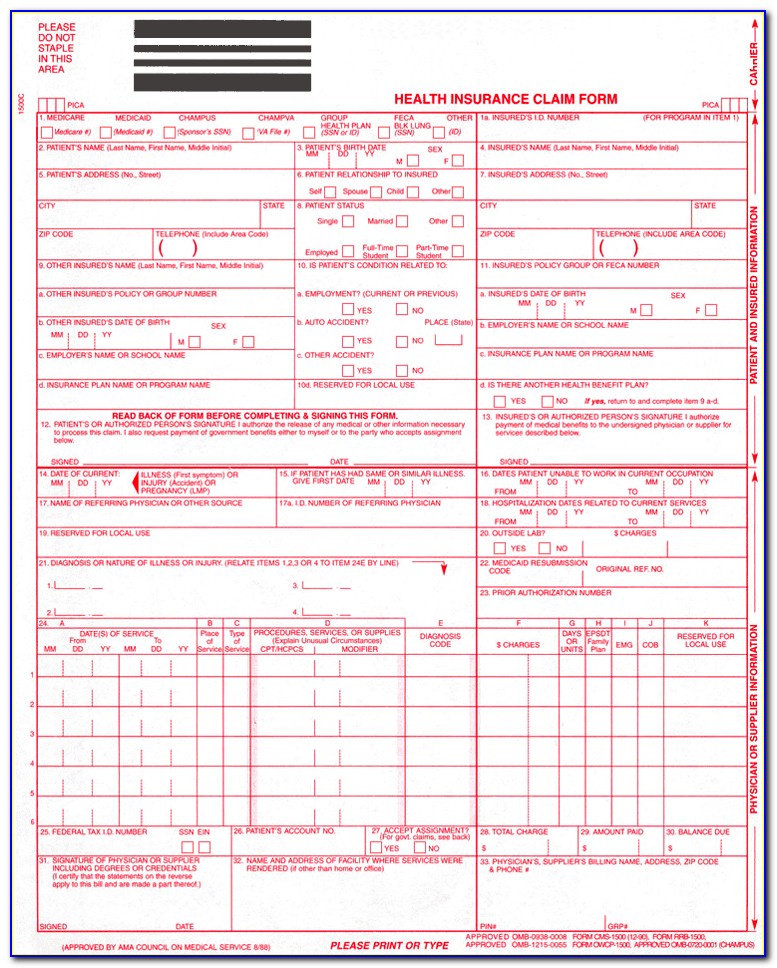
Health Insurance Claim Form Cms 1500 Instructions Form Resume
Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Number (for program in item 1) 4. Web cms 1500 dynamic list information. Failure to furnish any other information, such as.
Cms 1500 Claim Form Fillable Download Free Form Resume Examples
Health insurance claim form 1. You can decide how often to. Number (for program in item 1) 4. Web cms 1500 dynamic list information. Insured’s name (last name, first name, middle initial).
Medical Claim Form 1500 templates free printable
Number (for program in item 1) 4. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Medicare medicaid champus champva other read back of form before completing & signing this form. Please print or type form hcfa. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac),.

Medical Claim Form Cms 1500 Form Resume Examples 023dbqk1N5
Medicare medicaid tricare champva other read back of form before completing & signing this form. Read the instructions and tips below first. Please print or type form hcfa. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Claims may be electronically submitted to a medicare carrier, durable medical.
Medical Claim Form 1500 templates free printable
Medicare medicaid champus champva other read back of form before completing & signing this form. Web cms 1500 dynamic list information. Failure to furnish any other information, such as name or claim number, would delay payment of the claim. Failure to provide medical information under feca could be deemed an obstruction. Health insurance claim form 1.
Nucc 1500 Claim Form Form Resume Examples v19xN6yZV7
Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Medicare medicaid champus champva other read back of form before completing & signing this form. Failure to furnish any other information,.
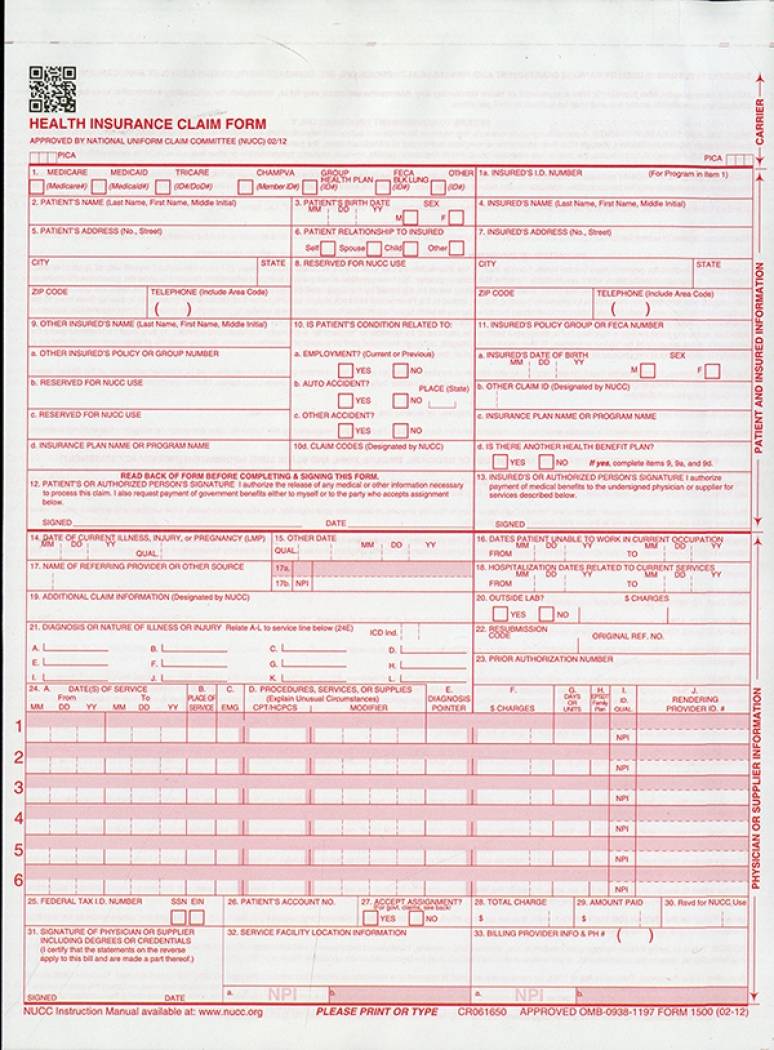
Health Insurance Claim Forms (CMS1500) 1part Continuation (2012
Please print or type form hcfa. Medicare medicaid champus champva other read back of form before completing & signing this form. Read the instructions and tips below first. Web health insurance claim form 1. Failure to provide medical information under feca could be deemed an obstruction.
Fillable Form 1500 Health Insurance Claim Form printable pdf download
Download free cms 1500 claim form fillable template. Sign up to get the latest information about your choice of cms topics. Failure to provide medical information under feca could be deemed an obstruction. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. You can decide how often to.
Web Health Insurance Claim Form 1.
The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Medicare medicaid champus champva other read back of form before completing & signing this form. Please print or type form hcfa. You can decide how often to.
Sign Up To Get The Latest Information About Your Choice Of Cms Topics.
Download free cms 1500 claim form fillable template. Health insurance claim form 1. Get everything done in minutes. Web cms 1500 dynamic list information.
Failure To Furnish Any Other Information, Such As Name Or Claim Number, Would Delay Payment Of The Claim.
Failure to provide medical information under feca could be deemed an obstruction. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Patient’s or authorized person’s signature i authorize the release of any medical or other information necessary. Medicare medicaid tricare champva other read back of form before completing & signing this form.
Number (For Program In Item 1) 4.
Web health insurance claim form 1500 printable. Insured’s name (last name, first name, middle initial). Read the instructions and tips below first. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor.