Letter Medical Necessity Form
Letter Medical Necessity Form - The letter often includes relevant patient history, medical needs, and the duration of the treatment. Under internal revenue service (irs) rules, certain expenses are eligible for health care account reimbursement only when accompanied by a letter of medical necessity. Web cms forms list. Web a medical necessity form can also be called a letter of diagnosis from doctor. Web this form, including the certification of medical necessity. Notice of denial of medical coverage/payment (integrated denial notice) The following is a sample letter of medical necessity that can be customized based on your patient’s medical history and demographic information. The following provides access and/or information for many cms forms. The services or items must be under the list of eligible expenses proofed by the right authorities. When required, submit this completed form with your claim submission as additional documentation.
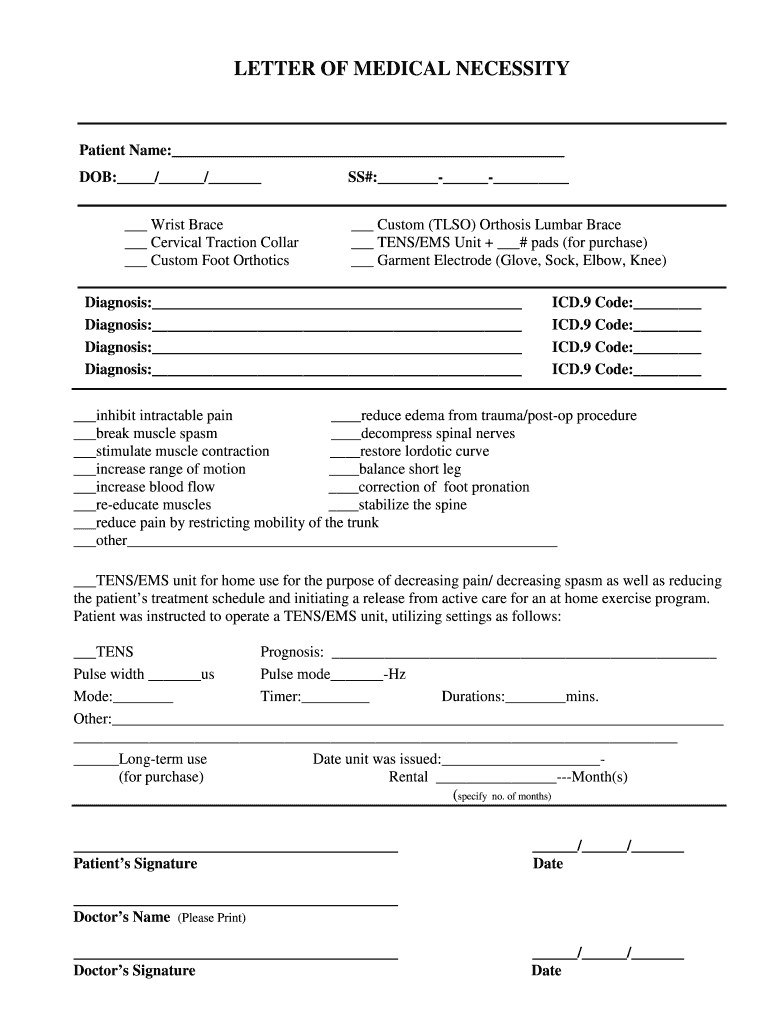
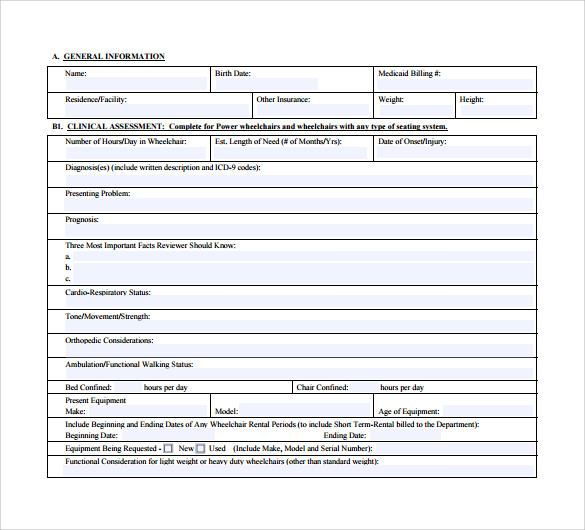
You may also use the search feature to more quickly locate information for a specific form number or form title. Web sample letter of medical necessity must be on the physician/providers letterhead please use the following guidelines when submitting a letter of medical necessity: Web a certificate of medical necessity (cmn) or a dme information form (dif) is a form required to help document the medical necessity and other coverage criteria for selected durable medical equipment, prosthetics, orthotics, and supplies (dmepos) items. Web cms forms list. Notice of denial of medical coverage/payment (integrated denial notice) Web letter of medical necessity form form instructions: The diagnosis must be specific. The letter often includes relevant patient history, medical needs, and the duration of the treatment. The services or items must be under the list of eligible expenses proofed by the right authorities. By submitting the letter of medical necessity, you certify that the expenses you are claiming are a direct result of the medical condition described, and you would not incur the expenses if you were not treating this medical condition.
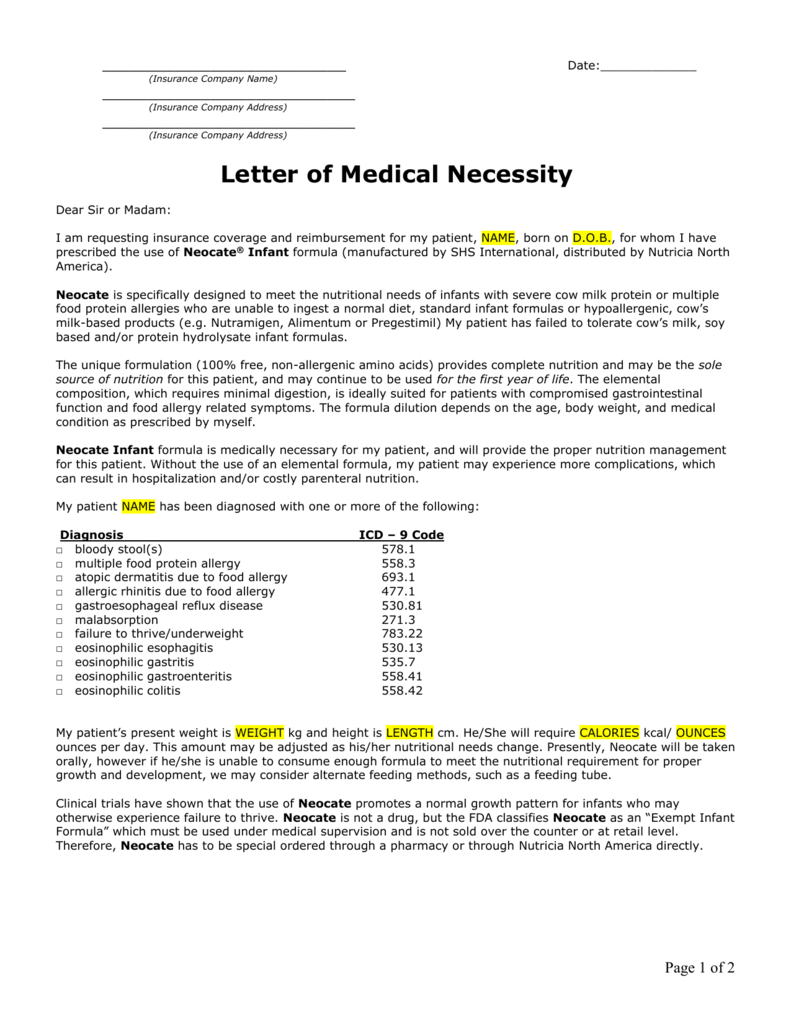
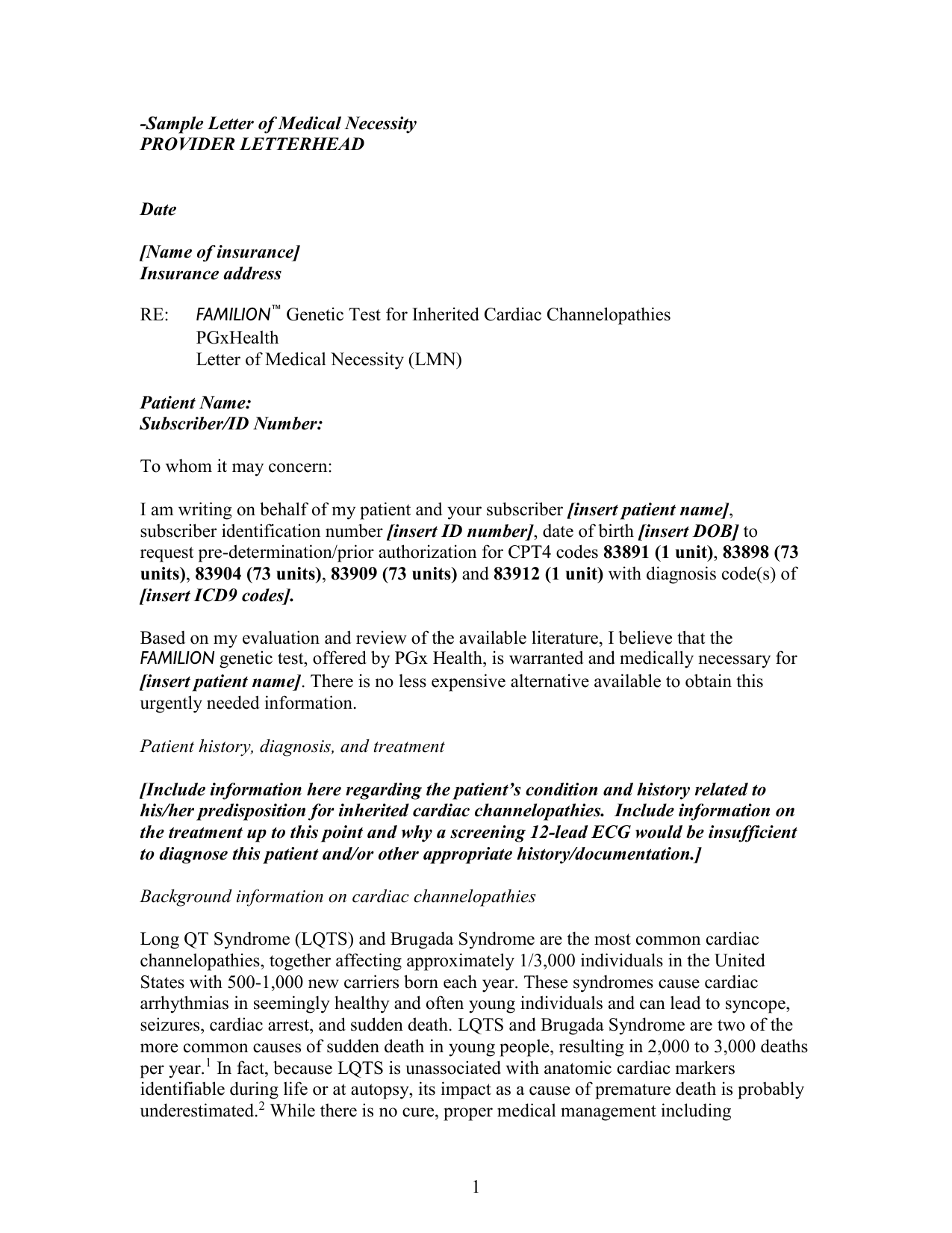
Web a patient‐specific letter of medical necessity will help to explain the physician’s rationale and clinical decision making in choosing a therapy. The following provides access and/or information for many cms forms. The letter often includes relevant patient history, medical needs, and the duration of the treatment. Web a letter of medical necessity (lomn) is a document from your licensed healthcare provider that recommends a particular treatment, product, or equipment for medical purposes. Web this form, including the certification of medical necessity. Web letter of medical necessity form form instructions: Web sample letter of medical necessity must be on the physician/providers letterhead please use the following guidelines when submitting a letter of medical necessity: Notice of denial of medical coverage/payment (integrated denial notice) The services or items must be under the list of eligible expenses proofed by the right authorities. By submitting the letter of medical necessity, you certify that the expenses you are claiming are a direct result of the medical condition described, and you would not incur the expenses if you were not treating this medical condition.
Medical Necessity Form Fill Out and Sign Printable PDF Template signNow
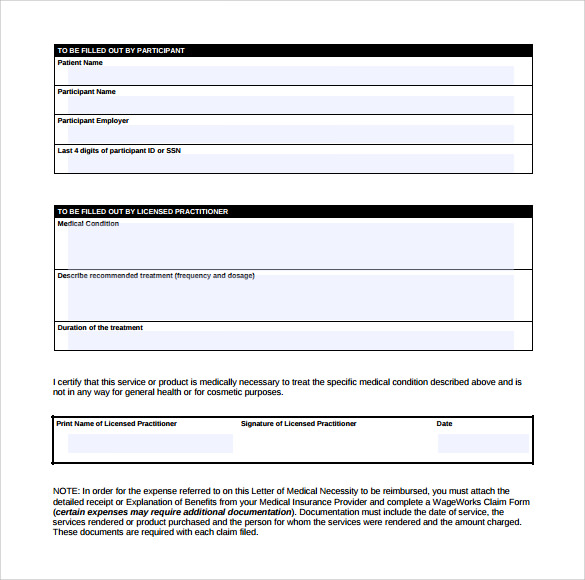
Web letter of medical necessity your medical care provider must complete this form for any service or product that falls under the category of “maybe expense” or “ineligible expense” per irc sec 213 (d) (1) if your provider believes the service or purchase is medically necessary for you or your eligible dependent(s). When required, submit this completed form with your.

Letter Of Medical Necessity Hsa Sample Cover Letters
Web cms forms list. Web letter of medical necessity form form instructions: Web letter of medical necessity your medical care provider must complete this form for any service or product that falls under the category of “maybe expense” or “ineligible expense” per irc sec 213 (d) (1) if your provider believes the service or purchase is medically necessary for you.
Letter of Medical Necessity
Web a letter of medical necessity (lomn) is a document from your licensed healthcare provider that recommends a particular treatment, product, or equipment for medical purposes. Web a certificate of medical necessity (cmn) or a dme information form (dif) is a form required to help document the medical necessity and other coverage criteria for selected durable medical equipment, prosthetics, orthotics,.
Sample Letter of Medical Necessity
Web a certificate of medical necessity (cmn) or a dme information form (dif) is a form required to help document the medical necessity and other coverage criteria for selected durable medical equipment, prosthetics, orthotics, and supplies (dmepos) items. The services or items must be under the list of eligible expenses proofed by the right authorities. Web a medical necessity form.

letter Letter Of Medical Necessity Template of medical necessity
Web a letter of medical necessity (lomn) is a document from your licensed healthcare provider that recommends a particular treatment, product, or equipment for medical purposes. The services or items must be under the list of eligible expenses proofed by the right authorities. When required, submit this completed form with your claim submission as additional documentation. Web a certificate of.
FREE 12+ Sample Letter of Medical Necessity Forms in PDF MS Word
Web a patient‐specific letter of medical necessity will help to explain the physician’s rationale and clinical decision making in choosing a therapy. The services or items must be under the list of eligible expenses proofed by the right authorities. Web cms forms list. Web sample letter of medical necessity must be on the physician/providers letterhead please use the following guidelines.

Letter Of Medical Necessity Form 2021 iammaslowmo
It verifies the medical services you are receiving and the items you are purchasing. Web a medical necessity form can also be called a letter of diagnosis from doctor. Notice of denial of medical coverage/payment (integrated denial notice) The following is a sample letter of medical necessity that can be customized based on your patient’s medical history and demographic information..
FREE 12+ Sample Letter of Medical Necessity Forms in PDF MS Word
Under internal revenue service (irs) rules, certain expenses are eligible for health care account reimbursement only when accompanied by a letter of medical necessity. When required, submit this completed form with your claim submission as additional documentation. Web a letter of medical necessity (lomn) is a document from your licensed healthcare provider that recommends a particular treatment, product, or equipment.

Letter Of Medical Necessity For Dme 20202022 Fill and Sign Printable
Web a patient‐specific letter of medical necessity will help to explain the physician’s rationale and clinical decision making in choosing a therapy. Under internal revenue service (irs) rules, certain expenses are eligible for health care account reimbursement only when accompanied by a letter of medical necessity. When required, submit this completed form with your claim submission as additional documentation. The.

Weight Loss Agreement Template Best of Document Template
By submitting the letter of medical necessity, you certify that the expenses you are claiming are a direct result of the medical condition described, and you would not incur the expenses if you were not treating this medical condition. The following is a sample letter of medical necessity that can be customized based on your patient’s medical history and demographic.
Web A Patient‐Specific Letter Of Medical Necessity Will Help To Explain The Physician’s Rationale And Clinical Decision Making In Choosing A Therapy.
Web letter of medical necessity form form instructions: Notice of denial of medical coverage/payment (integrated denial notice) Web cms forms list. The diagnosis must be specific.
Web This Form, Including The Certification Of Medical Necessity.
By submitting the letter of medical necessity, you certify that the expenses you are claiming are a direct result of the medical condition described, and you would not incur the expenses if you were not treating this medical condition. When required, submit this completed form with your claim submission as additional documentation. Web sample letter of medical necessity must be on the physician/providers letterhead please use the following guidelines when submitting a letter of medical necessity: The services or items must be under the list of eligible expenses proofed by the right authorities.
Download The Letter Of Medical Necessity Form (Pdf) , Complete The Form, Have Your Medical Provider Sign It, And Then Use Claim Submission Method That Works Best For You.
You may also use the search feature to more quickly locate information for a specific form number or form title. Under internal revenue service (irs) rules, certain expenses are eligible for health care account reimbursement only when accompanied by a letter of medical necessity. The letter often includes relevant patient history, medical needs, and the duration of the treatment. The following is a sample letter of medical necessity that can be customized based on your patient’s medical history and demographic information.
Web A Letter Of Medical Necessity (Lomn) Is A Document From Your Licensed Healthcare Provider That Recommends A Particular Treatment, Product, Or Equipment For Medical Purposes.
The following provides access and/or information for many cms forms. Web a certificate of medical necessity (cmn) or a dme information form (dif) is a form required to help document the medical necessity and other coverage criteria for selected durable medical equipment, prosthetics, orthotics, and supplies (dmepos) items. Web letter of medical necessity your medical care provider must complete this form for any service or product that falls under the category of “maybe expense” or “ineligible expense” per irc sec 213 (d) (1) if your provider believes the service or purchase is medically necessary for you or your eligible dependent(s). It verifies the medical services you are receiving and the items you are purchasing.