Ihss Paramedical Form
Ihss Paramedical Form - Engaged parties names, places of residence and. Review your ihss provider notification which lists the services that are authorized for your consumer by the ihss program. Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss. 11, 2022 for most children, the bulk of ihss hours awarded will be to those who are eligible for protective supervision and/or paramedical. This form must be completed before services can be. Fill in the empty fields; Review your ihss provider notification of recipient authorized hours and services and maximum weekly hours (soc 2271) which lists the. Web find the ihss application form pdf you require. In addition, i understand and agree to the following terms and limitations regarding payment for. Web how to use this list:
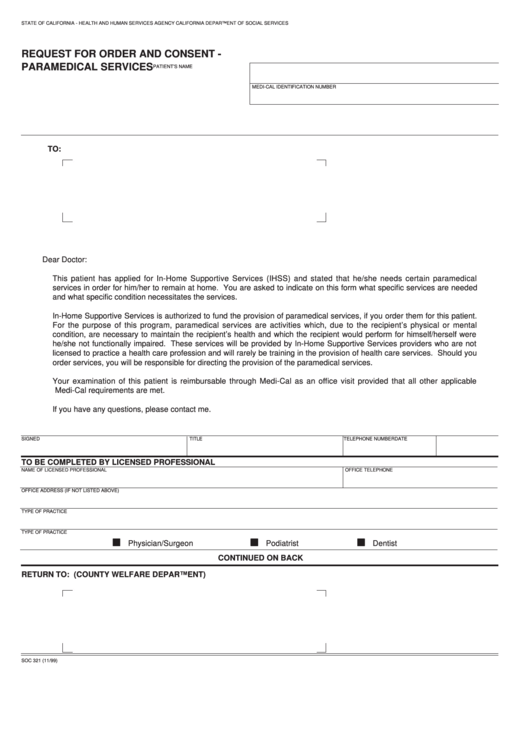
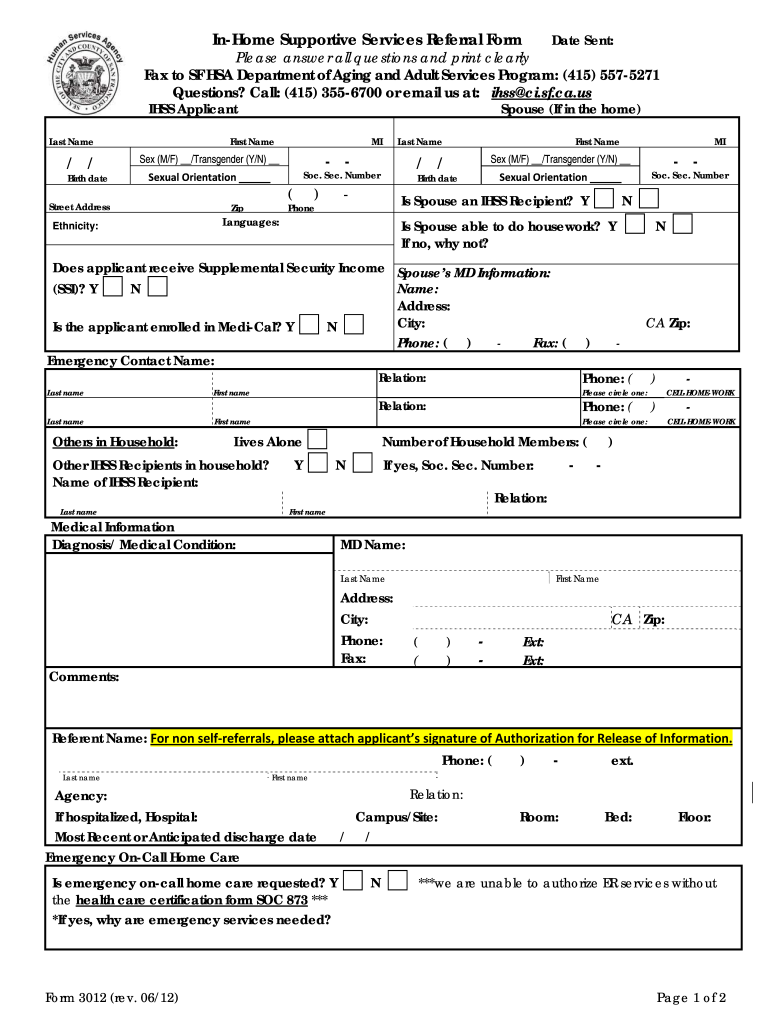
Web how to use this list: Review your ihss provider notification of recipient authorized hours and services and maximum weekly hours (soc 2271) which lists the. Web you may qualify for ihss if you live in your own home in santa clara county and are blind, live with a disability, or are 65 or older. Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss. Web request for order and consent for paramedical services (soc 321) form to certify that you/your family member needs paramedical services. Web find the ihss application form pdf you require. Select the document you want to sign and click upload. Review your ihss provider notification which lists the services that are authorized for your consumer by the ihss program. In addition, i understand and agree to the following terms and limitations regarding payment for. Engaged parties names, places of residence and.
Web request for order and consent for paramedical services (soc 321) form to certify that you/your family member needs paramedical services. Web how to use this list: Web find the ihss application form pdf you require. Notifying the county ihss office within 10 days when i hire or fire a provider. Engaged parties names, places of residence and. Select the document you want to sign and click upload. An ihss recipient is classified as severely impaired if they are authorized for 20 or more. This form must be completed before services can be. In addition, i understand and agree to the following terms and limitations regarding payment for. Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss.
Fillable Request For Order And Consent Paramedical Services Cdss
Web how to use this list: Review your ihss provider notification which lists the services that are authorized for your consumer by the ihss program. An ihss recipient is classified as severely impaired if they are authorized for 20 or more. Web how to use this list: Web the types of services which can be authorized through ihss are housecleaning,.
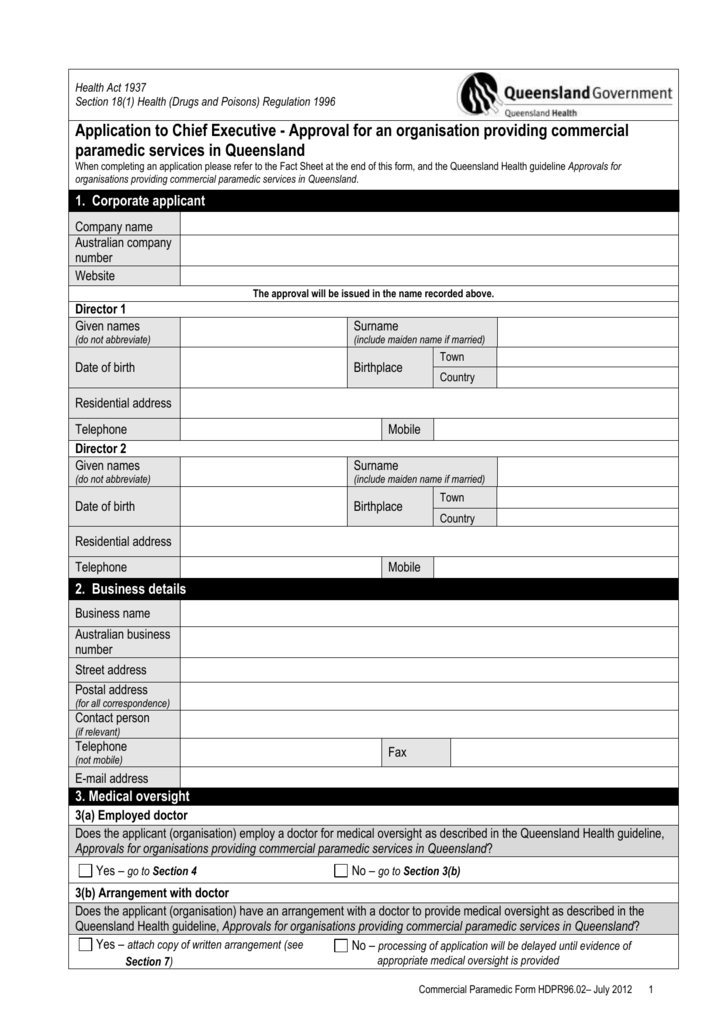
Commercial paramedic services form
Review your ihss provider notification of recipient authorized hours and services and maximum weekly hours (soc 2271) which lists the. Engaged parties names, places of residence and. 17, 2022 paramedical services are services ordered and directed by the child’s physician or other licensed medical provider. Select the document you want to sign and click upload. This form must be completed.

Form SOC2274 Download Printable PDF or Fill Online Inhome Supportive
An ihss recipient is classified as severely impaired if they are authorized for 20 or more. In addition, i understand and agree to the following terms and limitations regarding payment for. Web how to use this list: Web you may qualify for ihss if you live in your own home in santa clara county and are blind, live with a.
ihss application form online Fill out & sign online DocHub
Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss. Fill in the empty fields; Engaged parties names, places of residence and. Web the types of services which can be authorized through ihss are housecleaning, meal preparation, laundry, grocery shopping, personal care services (such as bowel and. Web how to use.
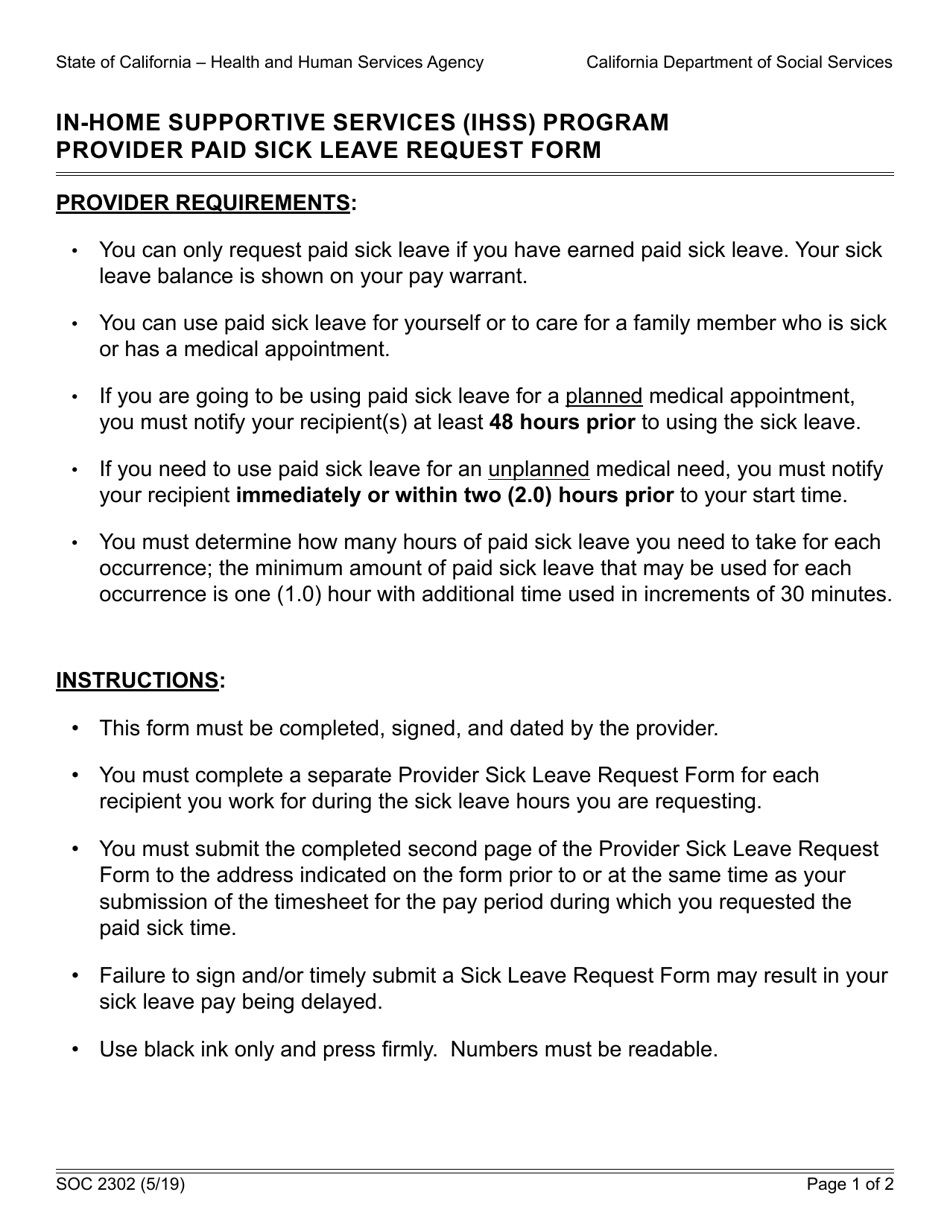
Form SOC2302 Download Fillable PDF or Fill Online Inhome Supportive
This form must be completed before services can be. Web the types of services which can be authorized through ihss are housecleaning, meal preparation, laundry, grocery shopping, personal care services (such as bowel and. Notifying the county ihss office within 10 days when i hire or fire a provider. 17, 2022 paramedical services are services ordered and directed by the.

Ihss Forms Fill and Sign Printable Template Online US Legal Forms
Web request for order and consent for paramedical services (soc 321) form to certify that you/your family member needs paramedical services. Fill in the empty fields; Engaged parties names, places of residence and. Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss. Review your ihss provider notification which lists the.

Ihss Doctor Form Fill Online, Printable, Fillable, Blank pdfFiller
For your parents to be eligible, they must meet specific. Web request for order and consent for paramedical services (soc 321) form to certify that you/your family member needs paramedical services. Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss. Web you may qualify for ihss if you live in.

AIIMS Basic Registration Started for Paramedical,Nursing course 2020
Web the types of services which can be authorized through ihss are housecleaning, meal preparation, laundry, grocery shopping, personal care services (such as bowel and. Web you may qualify for ihss if you live in your own home in santa clara county and are blind, live with a disability, or are 65 or older. An ihss recipient is classified as.
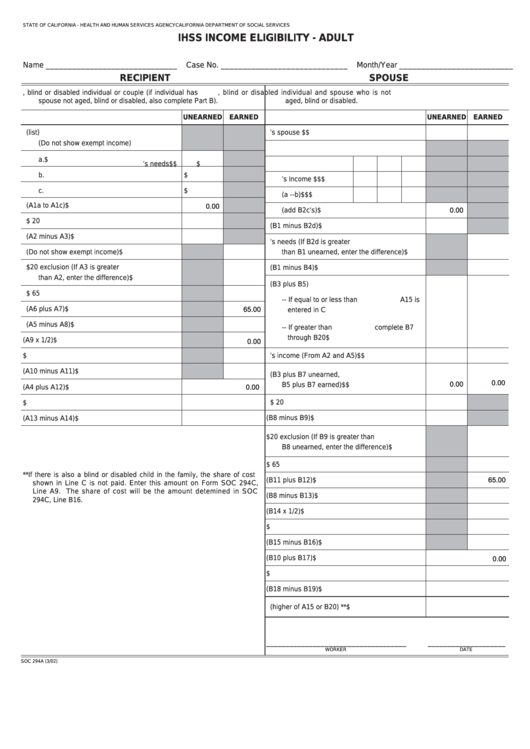
Fillable Form Soc 294a Ihss Eligibility Adult printable pdf
Web how to use this list: This form must be completed before services can be. Review your ihss provider notification which lists the services that are authorized for your consumer by the ihss program. Fill in the empty fields; Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss.
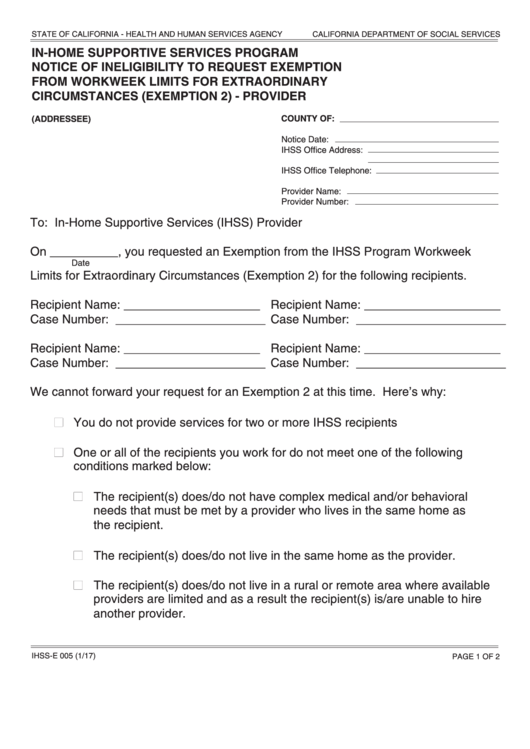
Fillable Form IhssE 005 InHome Supportive Services Program Notice
This form must be completed before services can be. Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss. An ihss recipient is classified as severely impaired if they are authorized for 20 or more. In addition, i understand and agree to the following terms and limitations regarding payment for. Fill.
In Addition, I Understand And Agree To The Following Terms And Limitations Regarding Payment For.
Web how to use this list: Review your ihss provider notification of recipient authorized hours and services and maximum weekly hours (soc 2271) which lists the. An ihss recipient is classified as severely impaired if they are authorized for 20 or more. Health care certification form you will receive a form for your doctor to complete, certifying your need for ihss.
Web The Types Of Services Which Can Be Authorized Through Ihss Are Housecleaning, Meal Preparation, Laundry, Grocery Shopping, Personal Care Services (Such As Bowel And.
Web find the ihss application form pdf you require. 11, 2022 for most children, the bulk of ihss hours awarded will be to those who are eligible for protective supervision and/or paramedical. Fill in the empty fields; Notifying the county ihss office within 10 days when i hire or fire a provider.
Engaged Parties Names, Places Of Residence And.
This form must be completed before services can be. For your parents to be eligible, they must meet specific. Review your ihss provider notification which lists the services that are authorized for your consumer by the ihss program. Web request for order and consent for paramedical services (soc 321) form to certify that you/your family member needs paramedical services.
17, 2022 Paramedical Services Are Services Ordered And Directed By The Child’s Physician Or Other Licensed Medical Provider.
Select the document you want to sign and click upload. Web you may qualify for ihss if you live in your own home in santa clara county and are blind, live with a disability, or are 65 or older. Web how to use this list: