Hmsa Prior Authorization Form Pdf
Hmsa Prior Authorization Form Pdf - Web the tips below will help you fill out hmsa prior authorization criteria form easily and quickly: Create professional documents with signnow. Use the tools in the. This patient’s benefit plan requires prior authorization for. Web hmsa behavioral health program utilization management (um) department prior authorization request phone number: To make an appropriate determination, providing the most. Web hmsa precertification request form please fax completed form to: How will providers and office staff request authorization for a physical medicine service? This patient’s benefit plan requires prior authorization for. Web prior authorization providers must request prior authorization for the physical medicine procedures listed below within 10 business days of the requested authorization start.
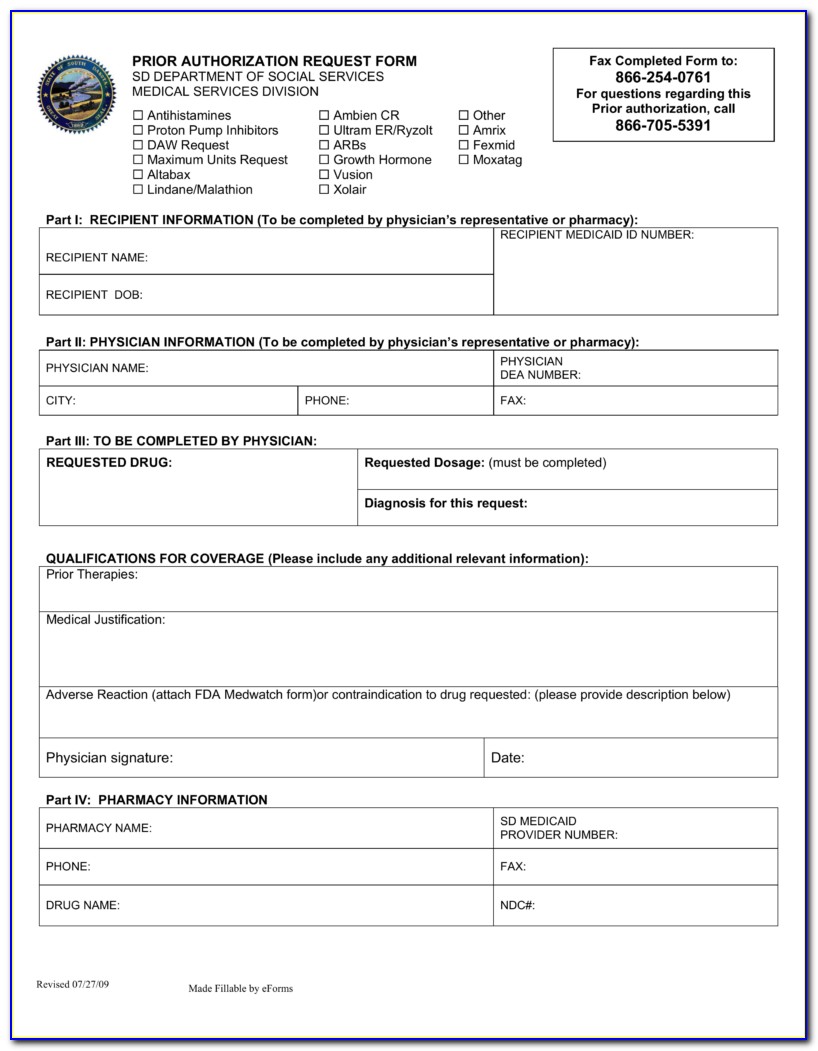
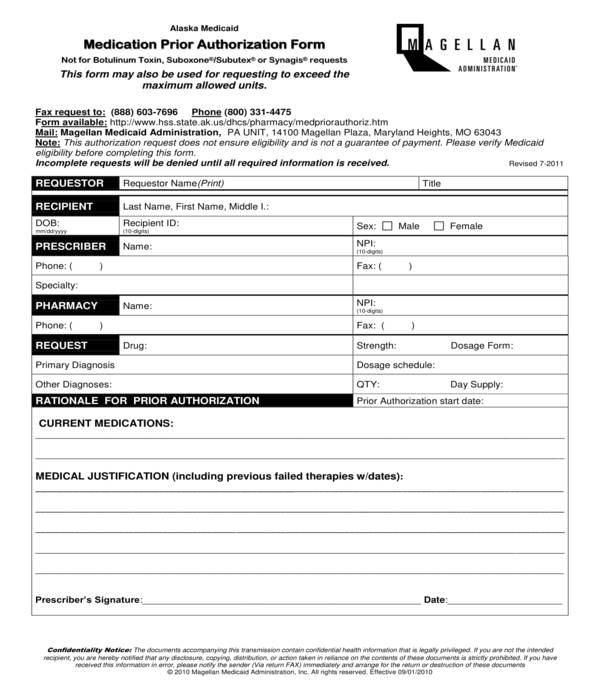
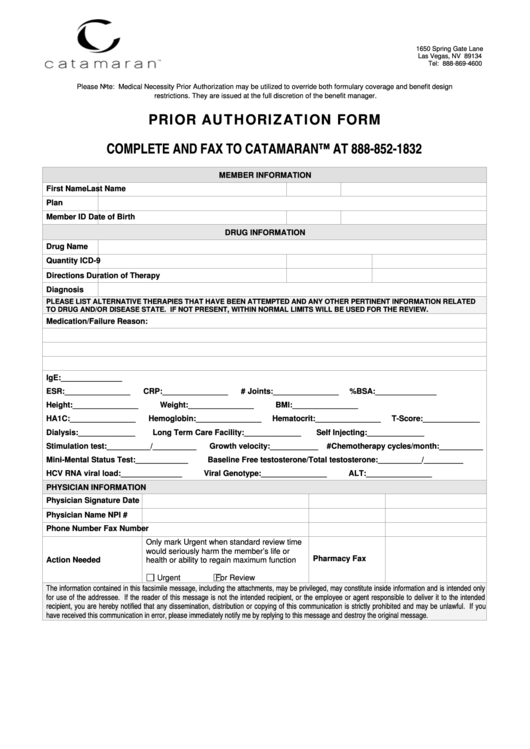
This patient’s benefit plan requires prior authorization for. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. Create professional documents with signnow. Hold on a second before the hmsa authorization form is loaded. Web up to $40 cash back hmsa form form hsa recertification request please fax completed form to: Web hmsa precertification request form please fax completed form to: Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. To make an appropriate determination, providing the most. Web click the get form or get form now button on the current page to access the pdf editor. _ patient information last name first name phone number gender m f date of birth / / member.
Web hmsa precertification request form please fax completed form to: Web hmsa behavioral health program utilization management (um) department prior authorization request phone number: To expedite the process, please have the following information ready before. Web hawaii standardized prescription drug prior authorization form* request date: Web up to $40 cash back hmsa form form hsa recertification request please fax completed form to: _ patient information last name first name phone number gender m f date of birth / / member. Web 1— prior authorization checklist (non cardiac) _hmsa 10/2017 prior authorization information. Web prior authorization providers must request prior authorization for the physical medicine procedures listed below within 10 business days of the requested authorization start. Web hmsa behavioral health program utilization management (um) department prior authorization request phone number: You will enter into our pdf editor.
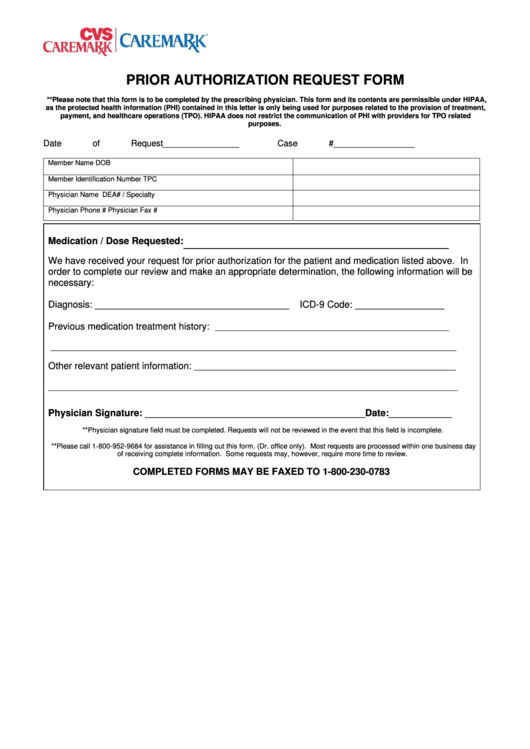
Caremark Prior Authorization Form printable pdf download
Create professional documents with signnow. Web click the get form or get form now button on the current page to access the pdf editor. This patient’s benefit plan requires prior authorization for. How to change and esign quest. This patient’s benefit plan requires prior authorization for.
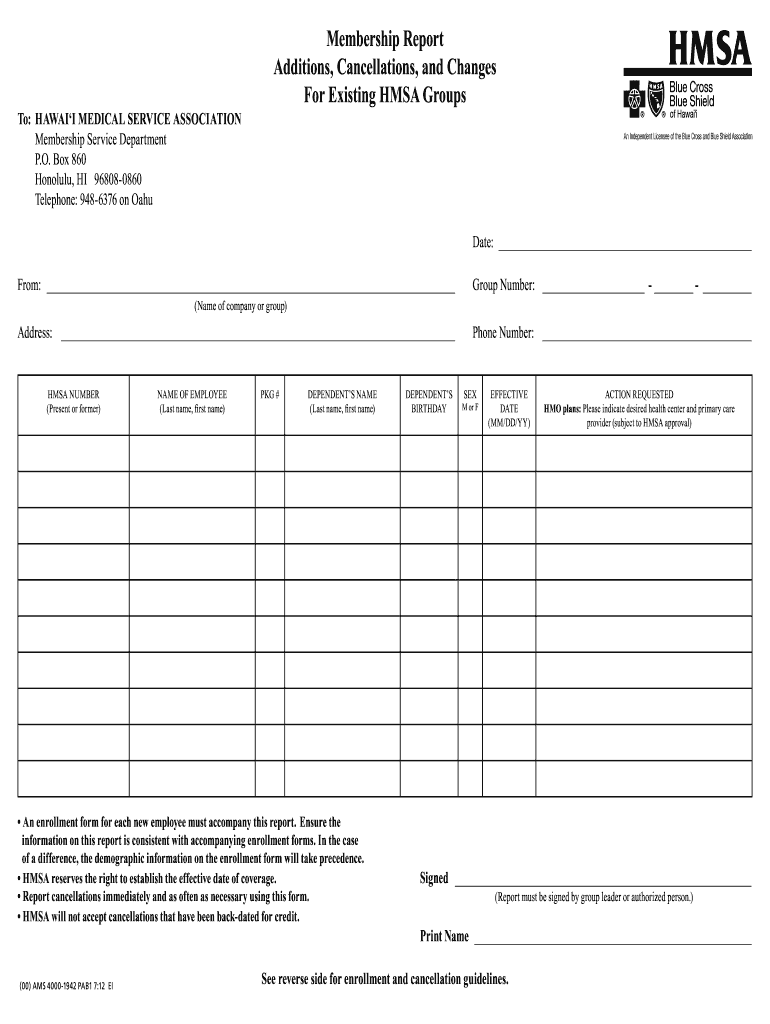
Hmsa Membership Report Form Fill Out and Sign Printable PDF Template
This patient’s benefit plan requires prior authorization for. Web the tips below will help you fill out hmsa prior authorization criteria form easily and quickly: Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. How will providers and office staff request authorization for a physical medicine service? Web prior authorization.
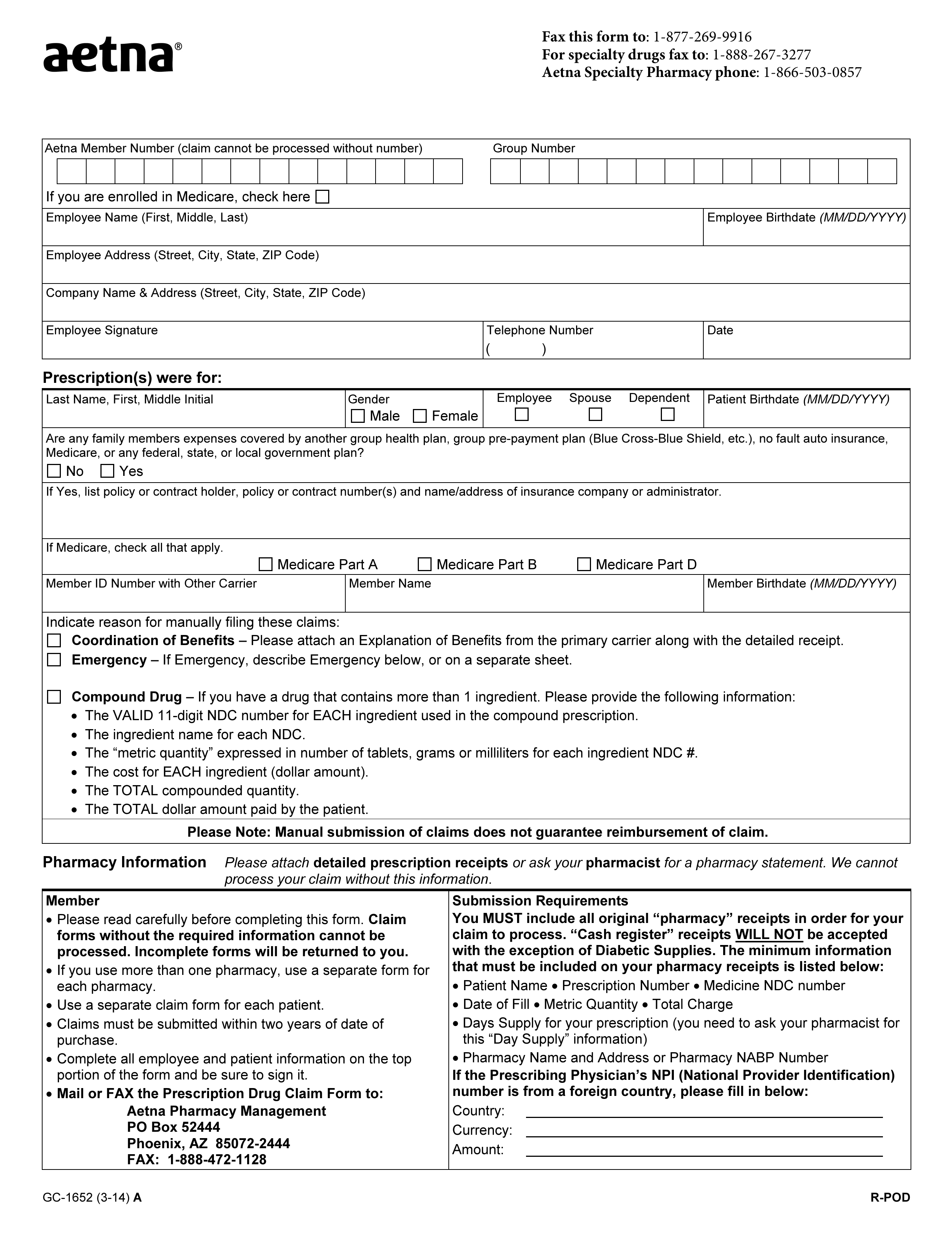
Free Aetna Prior (Rx) Authorization Form PDF eForms
You will enter into our pdf editor. Web follow these steps to get your hmsa precertification request form edited for the perfect workflow: Web click the get form or get form now button on the current page to access the pdf editor. Get your fillable template and complete it online using the instructions provided. Web prior authorization form instructions this.

ads/responsive.txt Health Net Prior Authorization form for Medication
Web hawaii standardized prescription drug prior authorization form* request date: This patient’s benefit plan requires prior authorization for. Web hmsa behavioral health program utilization management (um) department prior authorization request phone number: Web prior authorization form instructions this standardized prior authorization request form can be used for most prior authorization requests and use across all four health. Get your fillable.

Hmsa precertification form Fill out & sign online DocHub
To expedite the process, please have the following information ready before. Web follow these steps to get your hmsa precertification request form edited for the perfect workflow: Web physical medicine services don’t require prior authorization. How will providers and office staff request authorization for a physical medicine service? Web this patient’s benefit plan requires prior authorization for certain medications in.
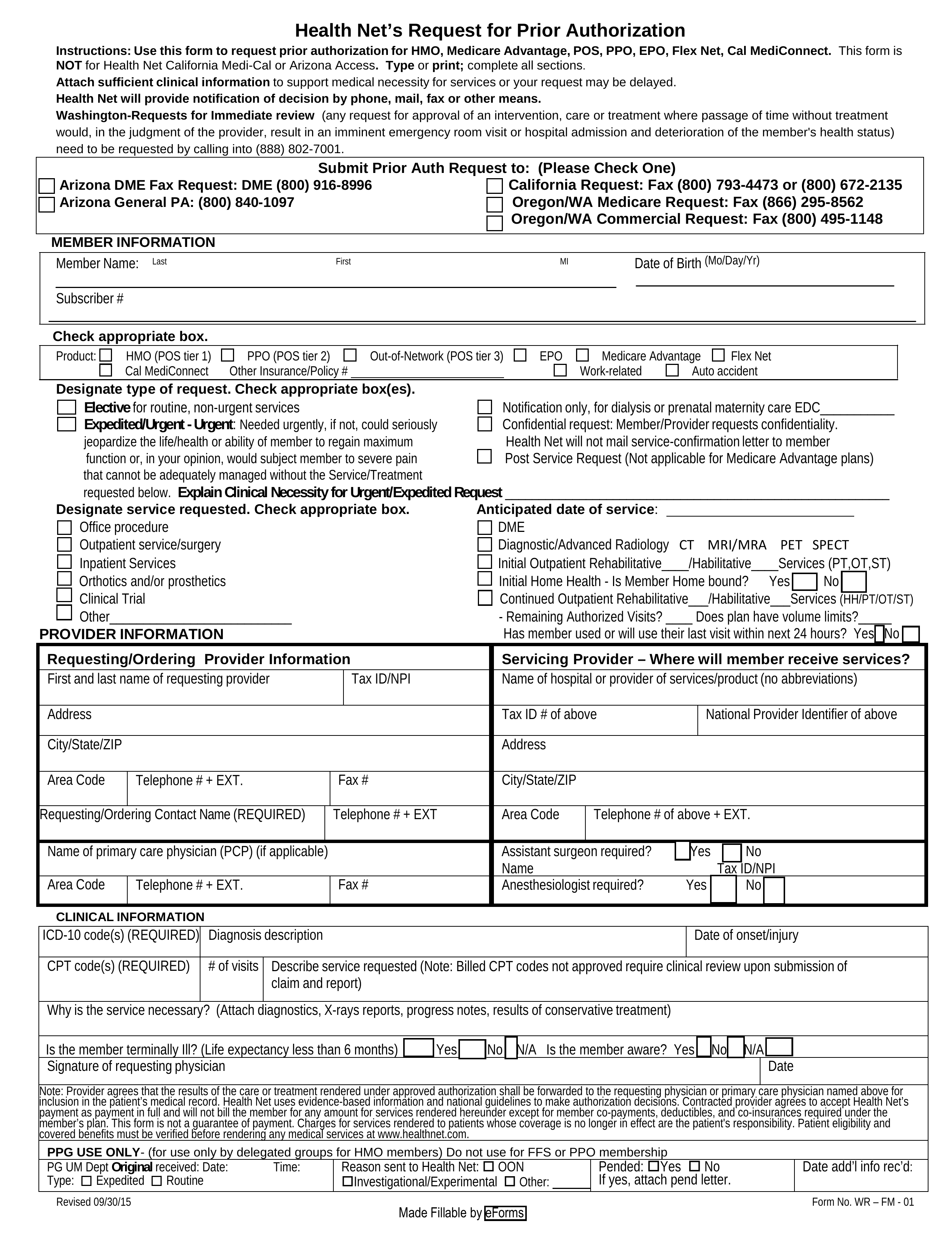
Free Health Net Prior (Rx) Authorization Form PDF eForms
Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. Web hmsa behavioral health program utilization management (um) department prior authorization request phone number: You will enter into our pdf editor. Create professional documents with signnow. _ patient information last name first name phone number gender m f date of birth.
Key.covermymeds Prior Authorization Form Form Resume Examples
To expedite the process, please have the following information ready before. Web prior authorization providers must request prior authorization for the physical medicine procedures listed below within 10 business days of the requested authorization start. Web hmsa behavioral health program utilization management (um) department prior authorization request phone number: Web this patient’s benefit plan requires prior authorization for certain medications.
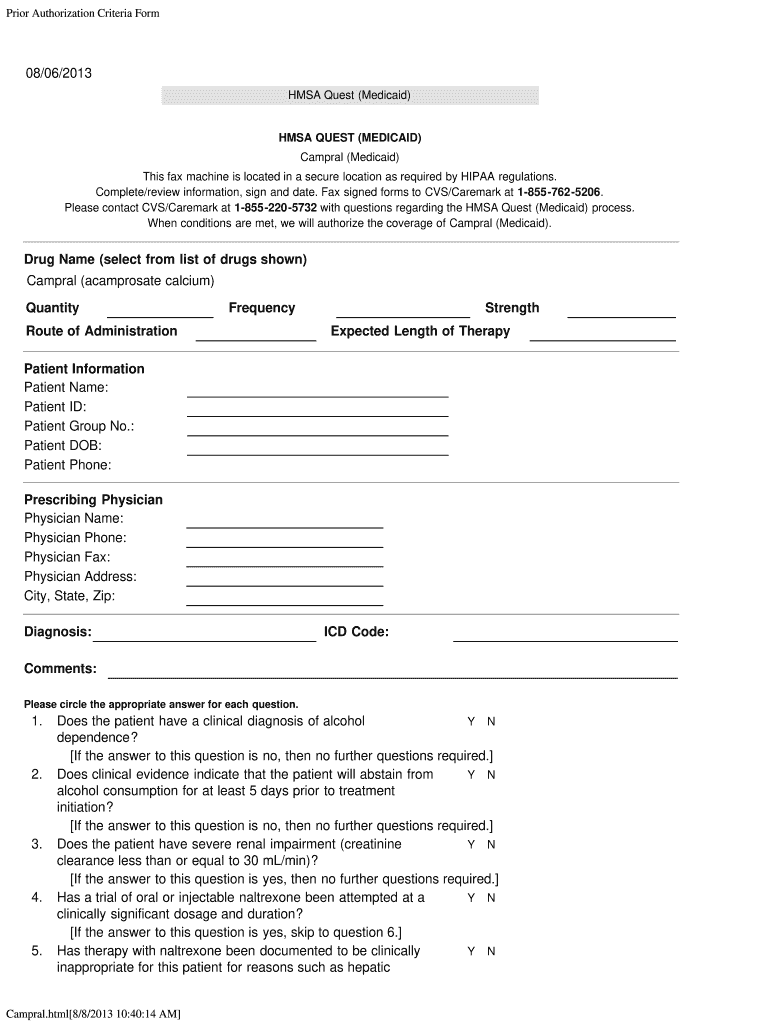
Authorization Medicaid Campral Fill Out and Sign Printable PDF
Web physical medicine services don’t require prior authorization. _ patient information last name first name phone number gender m f date of birth / / member. This patient’s benefit plan requires prior authorization for. Create professional documents with signnow. Web follow these steps to get your hmsa precertification request form edited for the perfect workflow:
FREE 11+ Prior Authorization Forms in PDF MS Word
To expedite the process, please have the following information ready before. This patient’s benefit plan requires prior authorization for. _ patient information last name first name phone number gender m f date of birth / / member. Select the get form button on this page. Web hawaii standardized prescription drug prior authorization form* request date:
Prior Authorization Form printable pdf download
Web follow these steps to get your hmsa precertification request form edited for the perfect workflow: Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. _ patient information last name first name phone number gender m f date of birth / / member. To expedite the process, please have the.
Web The Tips Below Will Help You Fill Out Hmsa Prior Authorization Criteria Form Easily And Quickly:
Web 1— prior authorization checklist (non cardiac) _hmsa 10/2017 prior authorization information. Web hmsa precertification request form please fax completed form to: Web click the get form or get form now button on the current page to access the pdf editor. This patient’s benefit plan requires prior authorization for.
Use The Tools In The.
To make an appropriate determination, providing the most. Web hmsa prior authorization form. Web prior authorization providers must request prior authorization for the physical medicine procedures listed below within 10 business days of the requested authorization start. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered.
You Will Enter Into Our Pdf Editor.
Web hmsa behavioral health program utilization management (um) department prior authorization request phone number: Create professional documents with signnow. Web follow these steps to get your hmsa precertification request form edited for the perfect workflow: Get your fillable template and complete it online using the instructions provided.
_ Patient Information Last Name First Name Phone Number Gender M F Date Of Birth / / Member.
Web hawaii standardized prescription drug prior authorization form* request date: How to change and esign quest. Web this patient’s benefit plan requires prior authorization for certain medications in order for the drug to be covered. To make an appropriate determination, providing the most.