Hcfa 1500 Printable Form
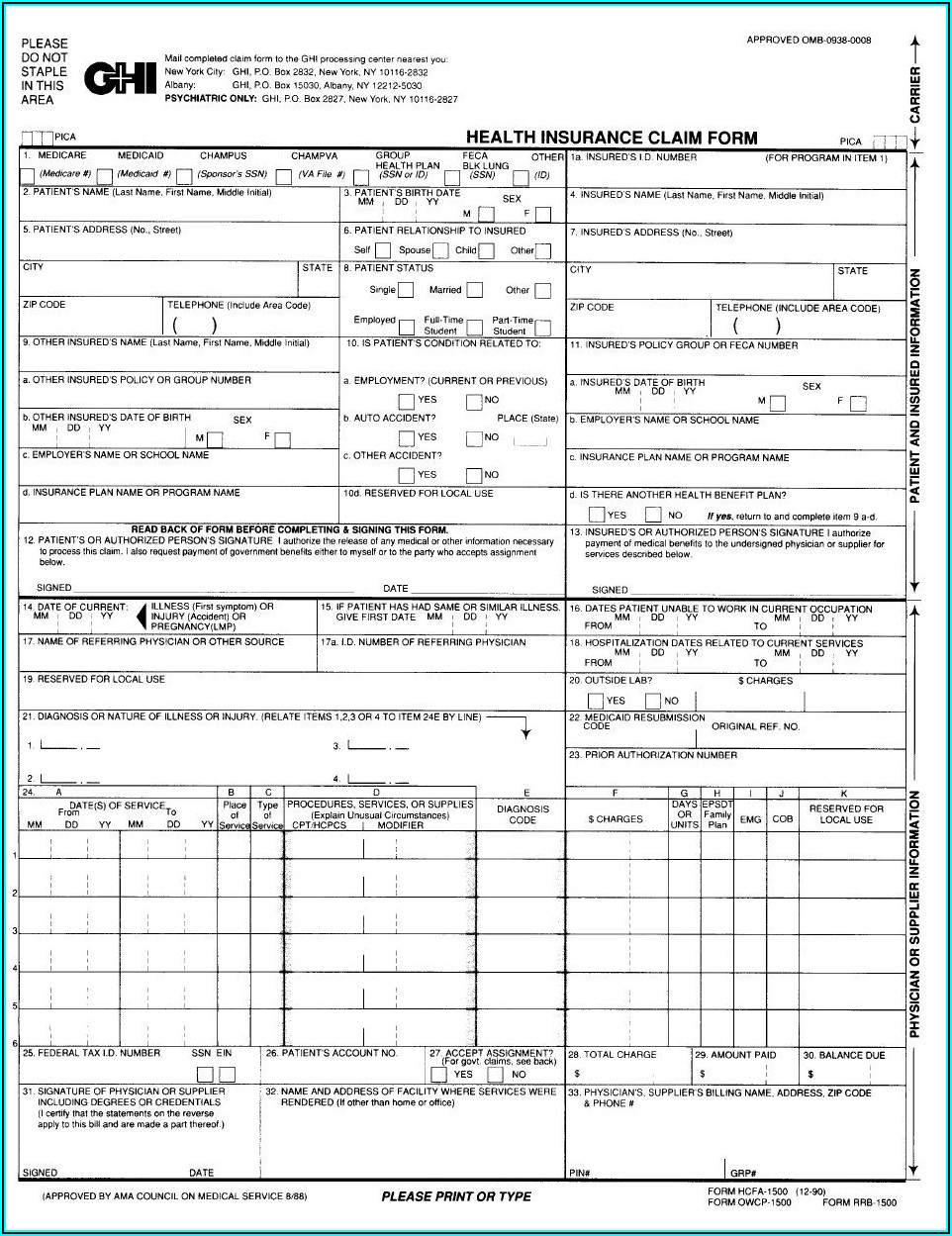
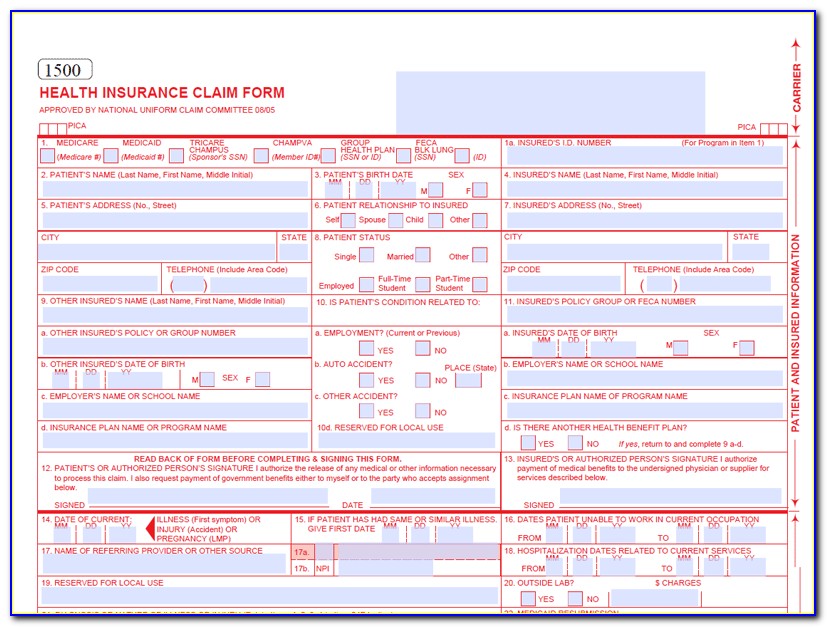
Hcfa 1500 Printable Form - Insured’s name (last name, first name, middle initial) 7. We are not affiliated with any brand or entity on this form. Number (for program in item 1) 4. Insured’s address (no., street) city state zip code telephone (include area code) 11. We are authorized by hcfa, champus. Web health insurance claim form health insurance claim form approved by national uniform claim committee medicare (medicare#) medicaid (medicaid#) tricare (id#/dod#) champva (member id#) group health plan (id#) feca blk lung (id#) other (id#) 1. Download free cms 1500 claim form fillable template. When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. Please mail them to the name and address listed here. Read the instructions and tips below first.
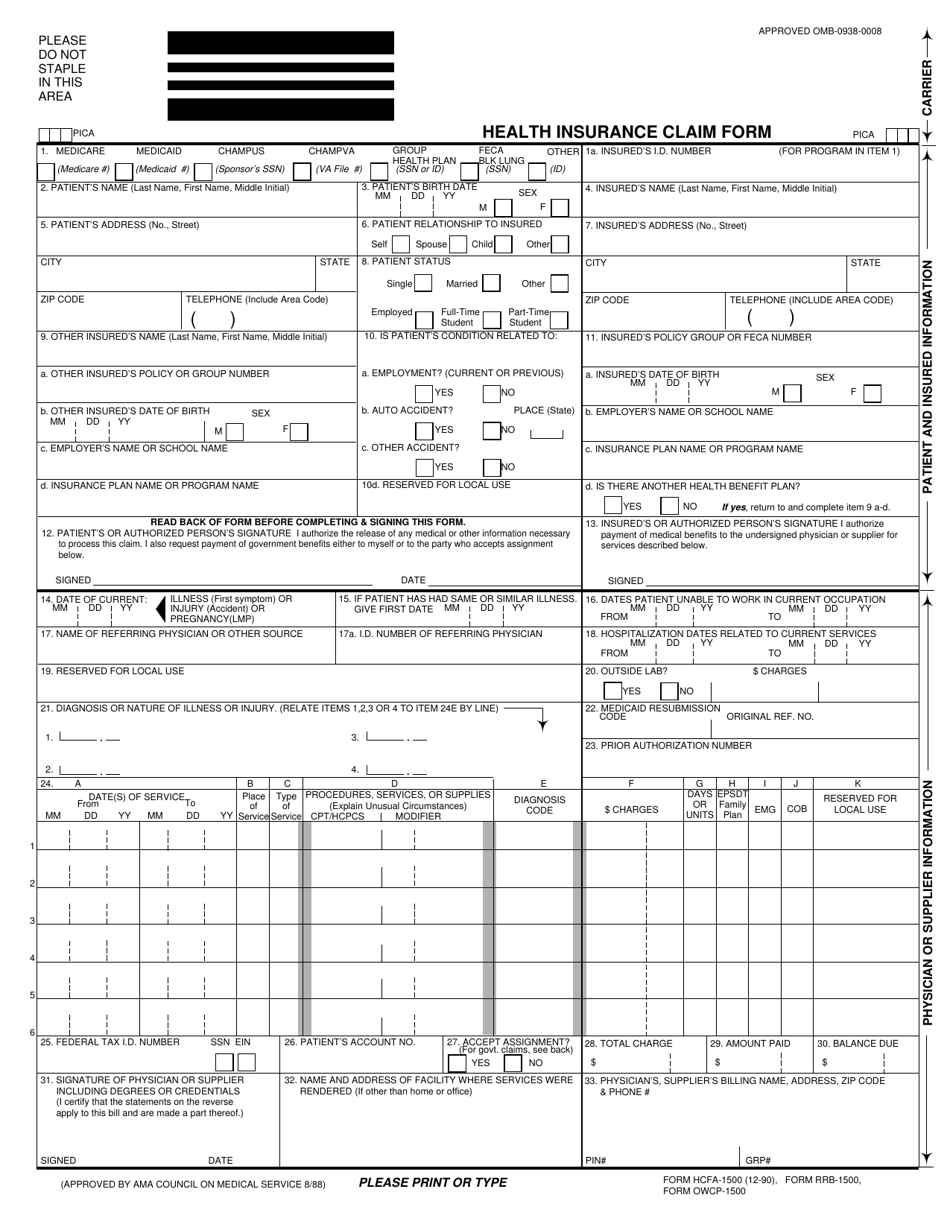
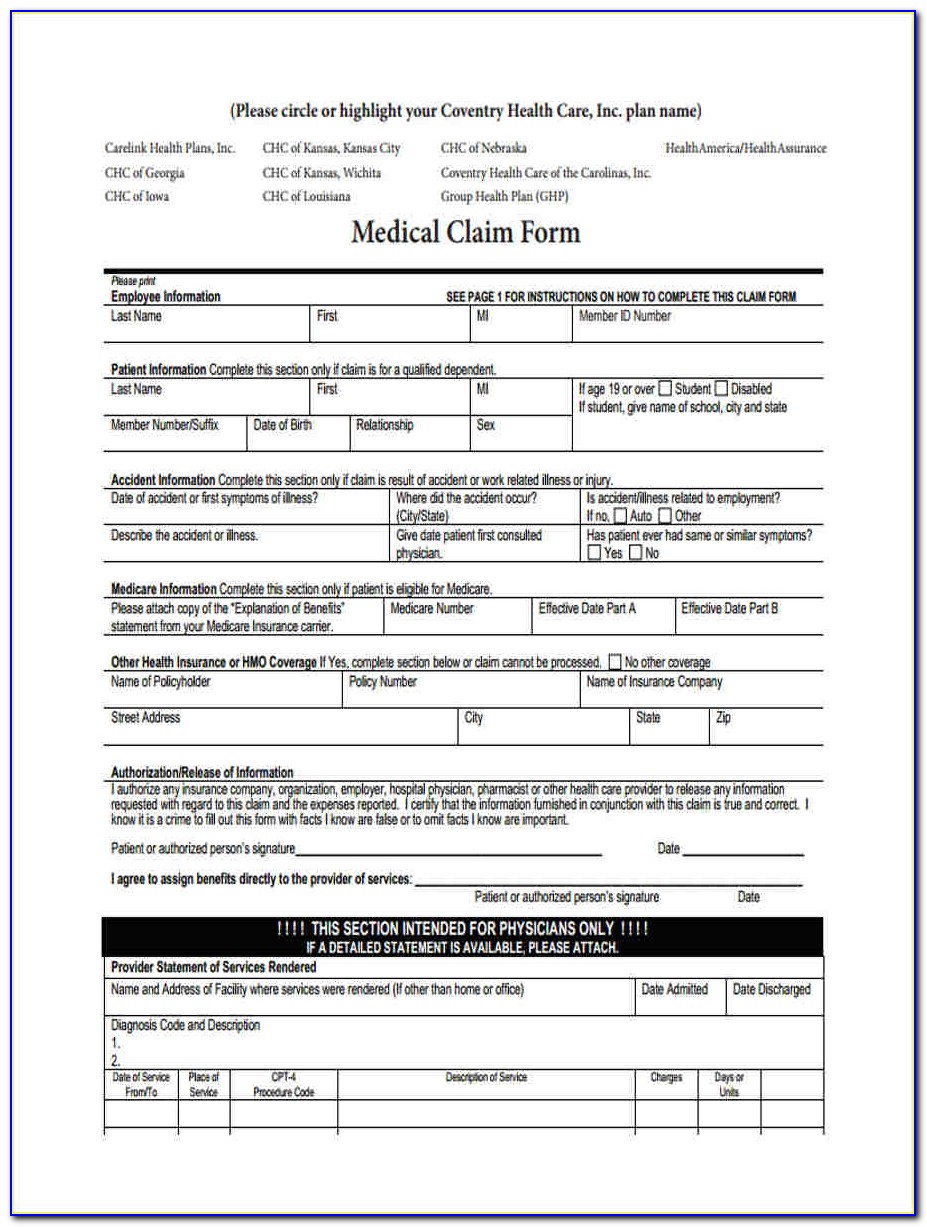
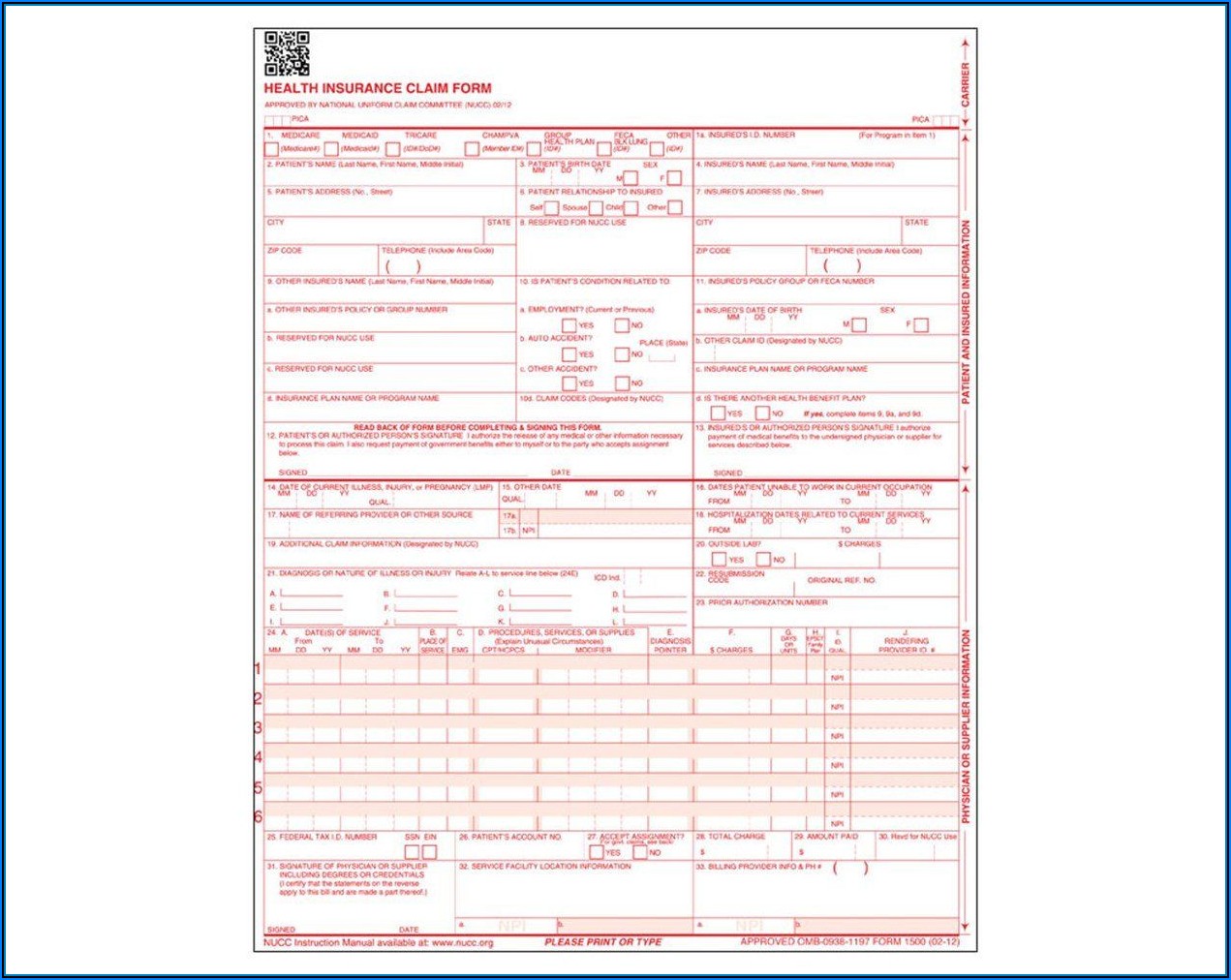
We are not affiliated with any brand or entity on this form. Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32). Web health insurance claim form health insurance claim form approved by national uniform claim committee medicare (medicare#) medicaid (medicaid#) tricare (id#/dod#) champva (member id#) group health plan (id#) feca blk lung (id#) other (id#) 1. We are authorized by hcfa, champus. Number (for program in item 1) 4. Insured’s address (no., street) city state zip code telephone (include area code) 11. Insured’s name (last name, first name, middle initial) 7. This could be through medicare, champus, group health care, or other forms of insurance. It is used to submit a bill or charge for health insurance coverage. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers.
Number (for program in item 1) 4. Read the instructions and tips below first. Please mail them to the name and address listed here. It is used for health care claims. Get the hcfa 1500 form printable 1990 template, fill it out, esign it, and share it in minutes. Sign up to get the latest information about your choice of cms topics. It is used to submit a bill or charge for health insurance coverage. Web cms 1500 dynamic list information. Web a hcfa 1500 form is used by the health care financing administration. Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32).
Form HCFA1500 Download Printable PDF or Fill Online Health Insurance
When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. Get the hcfa 1500 form printable 1990 template, fill it out, esign it, and share it in minutes. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Web cms 1500 dynamic list information. Any one.

Printable Hcfa 1500 Claim Form Form Resume Examples ygKzkewV3P
This could be through medicare, champus, group health care, or other forms of insurance. Insured’s name (last name, first name, middle initial) 7. Please mail them to the name and address listed here. Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. Sign up to get the latest information about.
How To Fill Out A Hcfa 1500 Form For Medicare Form Resume Examples
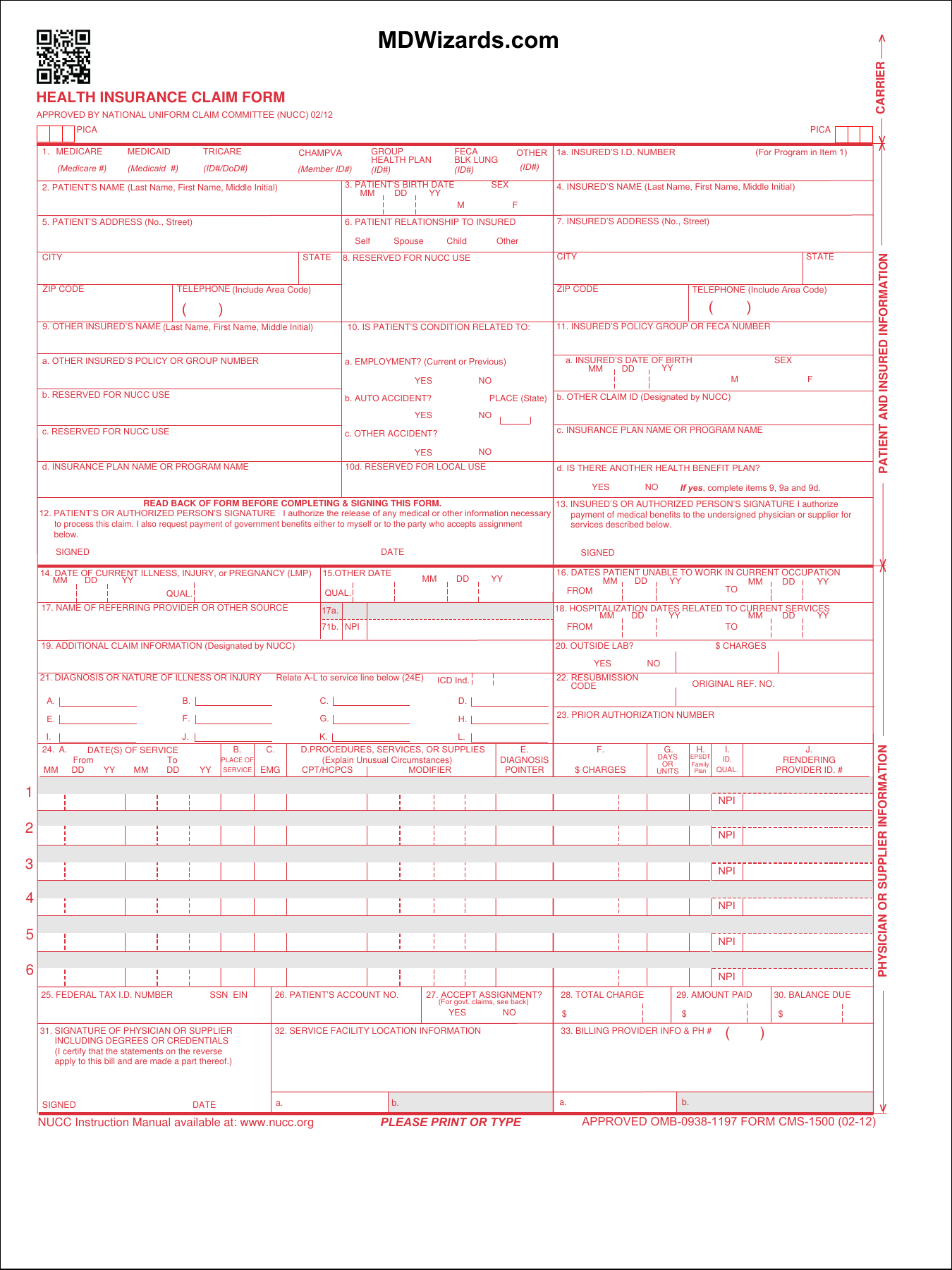
Read the instructions and tips below first. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. This could be through medicare,.
Free Hcfa 1500 Forms Printable Form Resume Examples yKVBjWMVMB
Web a hcfa 1500 form is used by the health care financing administration. It is used to submit a bill or charge for health insurance coverage. It is used for health care claims. Read the instructions and tips below first. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers,.

HCFA Forms, CMS 1500 Medical Forms, Health Insurance Claim Forms
Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. Insured’s address (no., street) city state zip code telephone (include area code) 11. When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. It is used for health care claims. Web health insurance claim.

Free Hcfa 1500 Form Form Resume Examples WjYDZMa2KB
It is used for health care claims. The 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Number (for program in item 1) 4. It is the basic paper claim form prescribed.
Printable Hcfa 1500 Claim Form Form Resume Examples pv9wXnJxY7
You can decide how often to. Get the hcfa 1500 form printable 1990 template, fill it out, esign it, and share it in minutes. When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. Web cms 1500 dynamic list information. Number (for program in item 1) 4.
Free Printable Hcfa 1500 Claim Form Form Resume Examples QBD3jjYkXn
We are not affiliated with any brand or entity on this form. It is used for health care claims. Web health insurance claim form health insurance claim form approved by national uniform claim committee medicare (medicare#) medicaid (medicaid#) tricare (id#/dod#) champva (member id#) group health plan (id#) feca blk lung (id#) other (id#) 1. We are authorized by hcfa, champus..

Free Hcfa 1500 Forms Printable Form Resume Examples dO3w67OKEn
Sign up to get the latest information about your choice of cms topics. Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. We are not affiliated with any brand or entity on this form. It is the basic paper claim form prescribed by many payers for claims submitted by physicians,.
Download Fillable HCFA 1500 Claim Form PDF RTF Word
Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. This could be through medicare, champus, group health care, or other forms of insurance. We are authorized by hcfa, champus. Read the instructions and tips below first. When you.
The 1500 Health Insurance Claim Form (1500 Claim Form) Answers The Needs Of Many Health Care Payers.
We are authorized by hcfa, champus. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Number (for program in item 1) 4. Sign up to get the latest information about your choice of cms topics.
We Are Not Affiliated With Any Brand Or Entity On This Form.
Get the hcfa 1500 form printable 1990 template, fill it out, esign it, and share it in minutes. Read the instructions and tips below first. Please mail them to the name and address listed here. Insured’s address (no., street) city state zip code telephone (include area code) 11.
You Can Decide How Often To.
Web a hcfa 1500 form is used by the health care financing administration. Download free cms 1500 claim form fillable template. It is the basic paper claim form prescribed by many payers for claims submitted by physicians, other providers, and suppliers, and in some cases, for ambulance services. Web health insurance claim form health insurance claim form approved by national uniform claim committee medicare (medicare#) medicaid (medicaid#) tricare (id#/dod#) champva (member id#) group health plan (id#) feca blk lung (id#) other (id#) 1.
Insured’s Name (Last Name, First Name, Middle Initial) 7.
Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. It is used to submit a bill or charge for health insurance coverage. It is used for health care claims. Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32).