Flu Vaccination Form
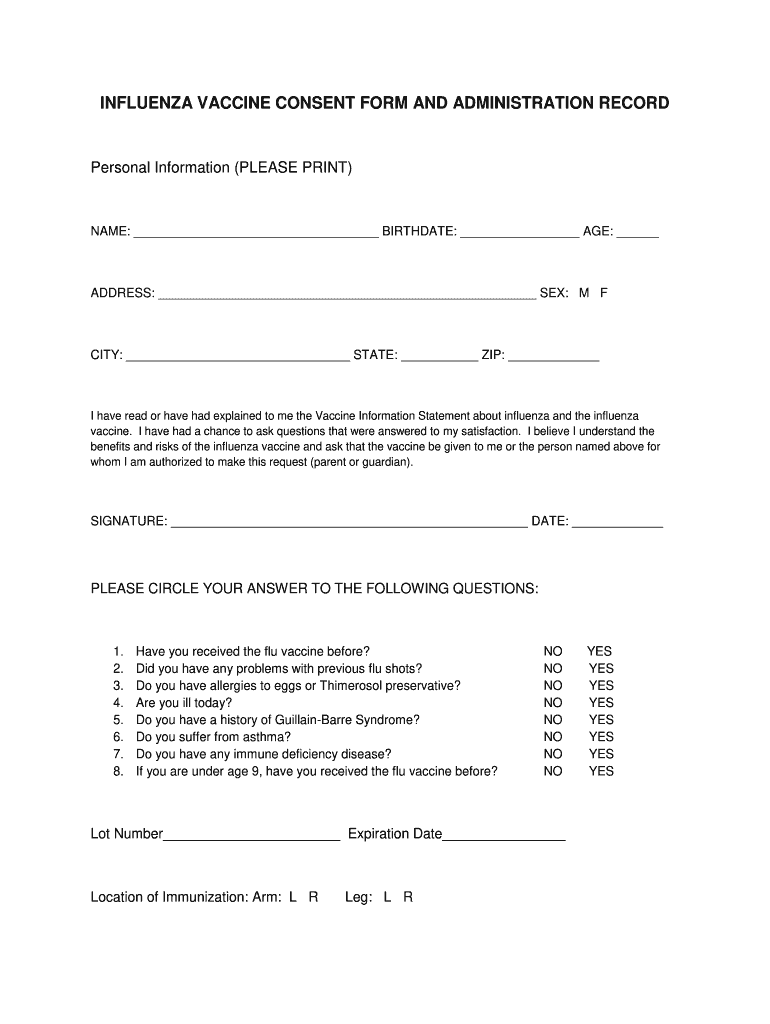
Flu Vaccination Form - Web influenza (flu) vaccines (often called “flu shots”) are vaccines that protect against the four influenza viruses that research indicates will be most common during the upcoming season. Do not have any of the conditions listed below: If i contract influenza, i can shed the virus for 24 hours before any influenza symptoms appear. _____/_____/____ (year, month, day) are you feeling ill today? Most flu vaccines are “flu shots” given with a needle, usually in the arm, but there also is a nasal spray flu vaccine. This record can be in electronic or paper form. No yes if yes, please explain below have you ever had a serious or an allergic reaction to a vaccine? Below are notes about each section on the template consent forms: Web document the vaccination (s) print. Serious reaction to previous flu vaccine.
This record can be in electronic or paper form. Web soreness, redness, and swelling where the shot is given, fever, muscle aches, and headache can happen after influenza vaccination. Health care providers who administer vaccines covered by the national childhood vaccine injury act are required to ensure that the permanent medical record. It should be signed by the patient, or, in the case of a minor, by a parent or legal guardian. Web vaccine, is this the first or second dose of seasonal influenza vaccine this year? Trainee, resident, intern, fee basis, or researcher) check one statement below and complete and sign the last section of this form prior to submission to employee occupational. Web health care personnel influenza vaccination form am a va: First second if second, please indicate the date of the first dose: Health care providers are required by law to record certain information in a patient’s medical record. Do not have any of the conditions listed below:
Most flu vaccines are “flu shots” given with a needle, usually in the arm, but there also is a nasal spray flu vaccine. Web influenza (flu) vaccines (often called “flu shots”) are vaccines that protect against the four influenza viruses that research indicates will be most common during the upcoming season. Health care providers who administer vaccines covered by the national childhood vaccine injury act are required to ensure that the permanent medical record. It should be signed by the patient, or, in the case of a minor, by a parent or legal guardian. Health care providers are required by law to record certain information in a patient’s medical record. Web soreness, redness, and swelling where the shot is given, fever, muscle aches, and headache can happen after influenza vaccination. This record can be in electronic or paper form. Web document the vaccination (s) print. _____/_____/____ (year, month, day) are you feeling ill today? If i contract influenza, i can shed the virus for 24 hours before any influenza symptoms appear.

Flu Vaccine Exemption Form All IU Campuses One.IU
Most flu vaccines are “flu shots” given with a needle, usually in the arm, but there also is a nasal spray flu vaccine. Do not have any of the conditions listed below: Trainee, resident, intern, fee basis, or researcher) check one statement below and complete and sign the last section of this form prior to submission to employee occupational. No.
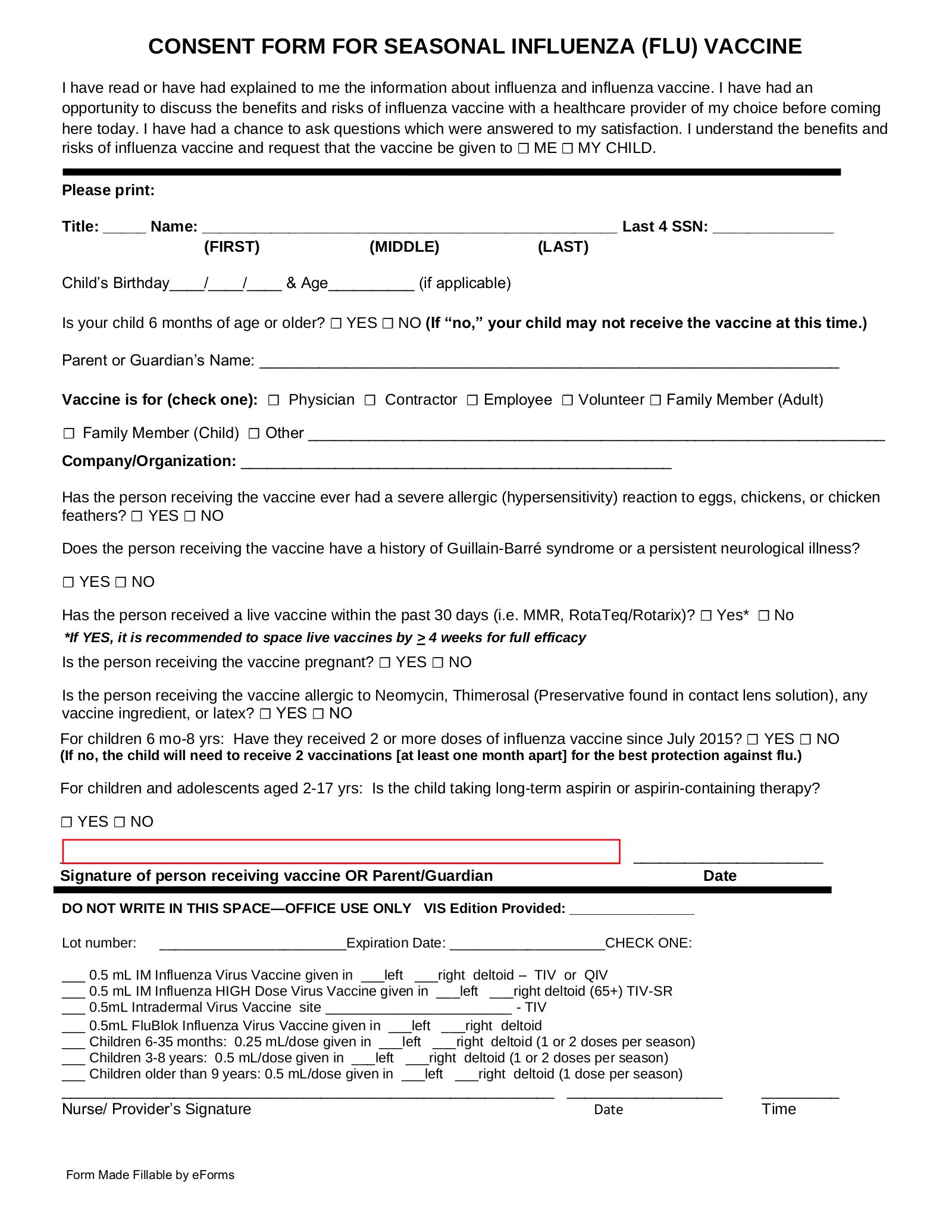
Free Flu Shot (Influenza) Vaccine Consent Form PDF Word eForms
Serious reaction to previous flu vaccine. This record can be in electronic or paper form. Web document the vaccination (s) print. Web influenza vaccination is recommended for me and all other healthcare personnel to protect our staff and our facility’s patients from influenza, its complications, and death. First second if second, please indicate the date of the first dose:
Flu Vaccine Consent Form 2019 2020 Fill Out and Sign Printable PDF
Most flu vaccines are “flu shots” given with a needle, usually in the arm, but there also is a nasal spray flu vaccine. If i contract influenza, i can shed the virus for 24 hours before any influenza symptoms appear. Web soreness, redness, and swelling where the shot is given, fever, muscle aches, and headache can happen after influenza vaccination..

20142015 Inactivated Influenza Vaccine Consent Form Free Download
_____/_____/____ (year, month, day) are you feeling ill today? Web soreness, redness, and swelling where the shot is given, fever, muscle aches, and headache can happen after influenza vaccination. It should be signed by the patient, or, in the case of a minor, by a parent or legal guardian. Web health care personnel influenza vaccination form am a va: Web.
Vaccine Consent Form Fill Out and Sign Printable PDF Template signNow
Most flu vaccines are “flu shots” given with a needle, usually in the arm, but there also is a nasal spray flu vaccine. If i contract influenza, i can shed the virus for 24 hours before any influenza symptoms appear. It should be signed by the patient, or, in the case of a minor, by a parent or legal guardian..
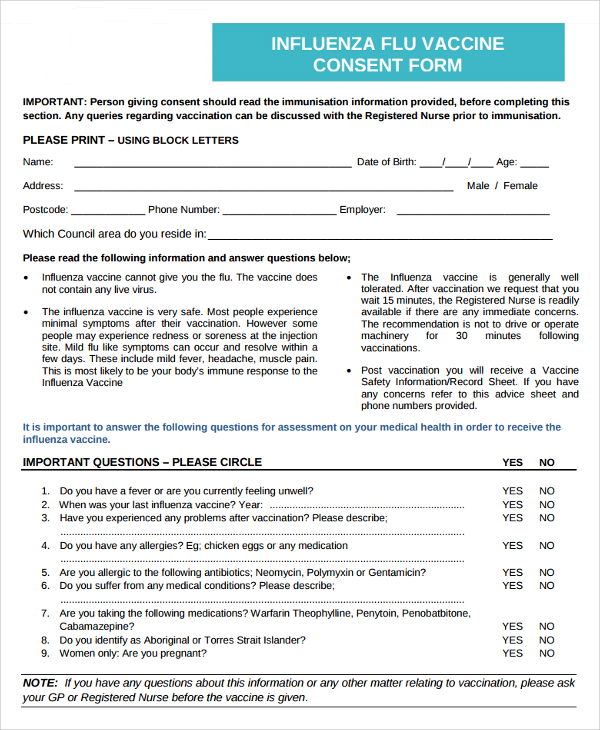
FREE 7+ Sample Vaccine Consent Forms in MS Word PDF
Web flu vaccine consent form 2022. Trainee, resident, intern, fee basis, or researcher) check one statement below and complete and sign the last section of this form prior to submission to employee occupational. Most flu vaccines are “flu shots” given with a needle, usually in the arm, but there also is a nasal spray flu vaccine. Do not have any.

Flu Vaccinations
Web health care personnel influenza vaccination form am a va: Serious reaction to previous flu vaccine. Web vaccine, is this the first or second dose of seasonal influenza vaccine this year? Health care providers who administer vaccines covered by the national childhood vaccine injury act are required to ensure that the permanent medical record. First second if second, please indicate.
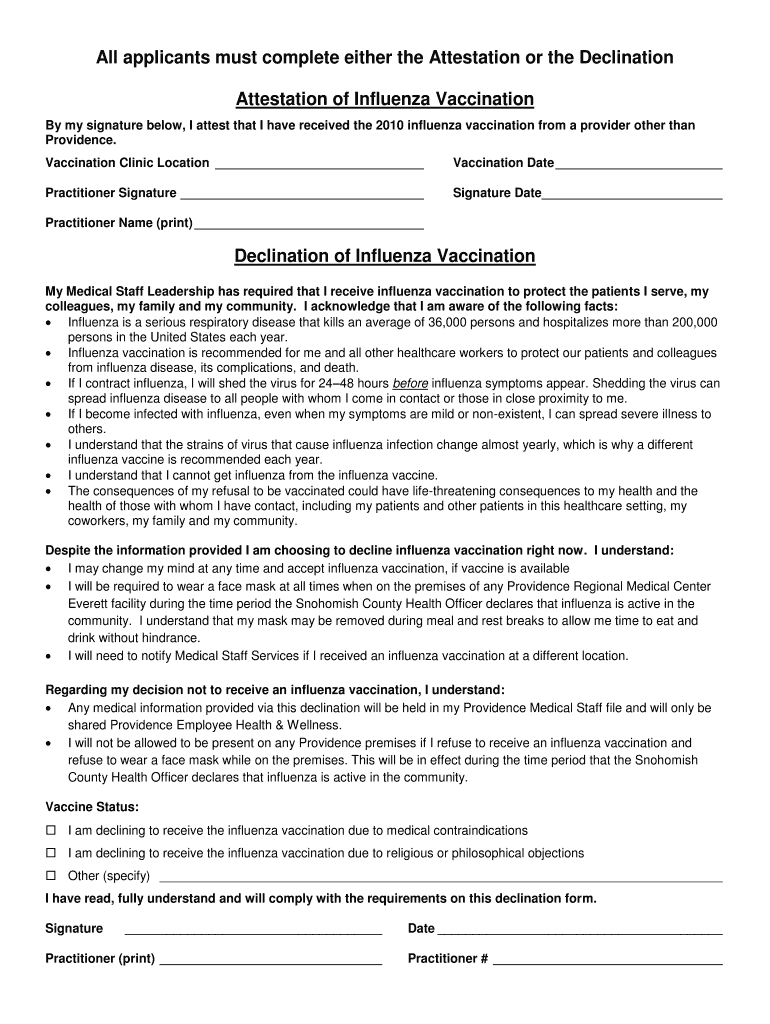
Flu Vaccine Consent Form Fill Out and Sign Printable PDF Template
No yes if yes, please explain below have you ever had a serious or an allergic reaction to a vaccine? Web influenza vaccination is recommended for me and all other healthcare personnel to protect our staff and our facility’s patients from influenza, its complications, and death. Do not have any of the conditions listed below: Web flu vaccine consent form.
Newcastle flu vaccine mixup leaves children unprotected BBC News
First second if second, please indicate the date of the first dose: Web influenza vaccination is recommended for me and all other healthcare personnel to protect our staff and our facility’s patients from influenza, its complications, and death. Trainee, resident, intern, fee basis, or researcher) check one statement below and complete and sign the last section of this form prior.

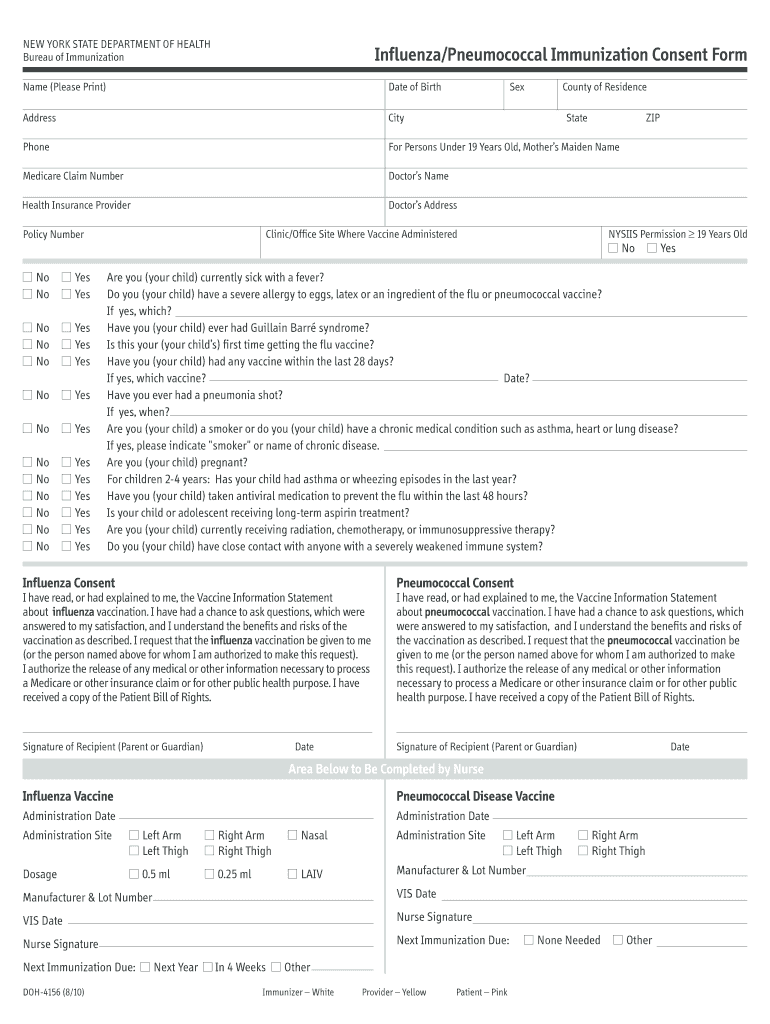
Patient Consent Form for Seasonal Influenza Vaccine Free Download
Web influenza (flu) vaccines (often called “flu shots”) are vaccines that protect against the four influenza viruses that research indicates will be most common during the upcoming season. Health care providers are required by law to record certain information in a patient’s medical record. Web vaccine, is this the first or second dose of seasonal influenza vaccine this year? Web.
Health Care Providers Who Administer Vaccines Covered By The National Childhood Vaccine Injury Act Are Required To Ensure That The Permanent Medical Record.
First second if second, please indicate the date of the first dose: No yes if yes, please explain below have you ever had a serious or an allergic reaction to a vaccine? If i contract influenza, i can shed the virus for 24 hours before any influenza symptoms appear. Web flu vaccine consent form 2022.
Web Health Care Personnel Influenza Vaccination Form Am A Va:
Trainee, resident, intern, fee basis, or researcher) check one statement below and complete and sign the last section of this form prior to submission to employee occupational. Web influenza vaccination is recommended for me and all other healthcare personnel to protect our staff and our facility’s patients from influenza, its complications, and death. Most flu vaccines are “flu shots” given with a needle, usually in the arm, but there also is a nasal spray flu vaccine. Below are notes about each section on the template consent forms:
Health Care Providers Are Required By Law To Record Certain Information In A Patient’s Medical Record.
Web soreness, redness, and swelling where the shot is given, fever, muscle aches, and headache can happen after influenza vaccination. Serious reaction to previous flu vaccine. Web document the vaccination (s) print. Web vaccine, is this the first or second dose of seasonal influenza vaccine this year?
Do Not Have Any Of The Conditions Listed Below:
Web influenza (flu) vaccines (often called “flu shots”) are vaccines that protect against the four influenza viruses that research indicates will be most common during the upcoming season. This record can be in electronic or paper form. It should be signed by the patient, or, in the case of a minor, by a parent or legal guardian. _____/_____/____ (year, month, day) are you feeling ill today?