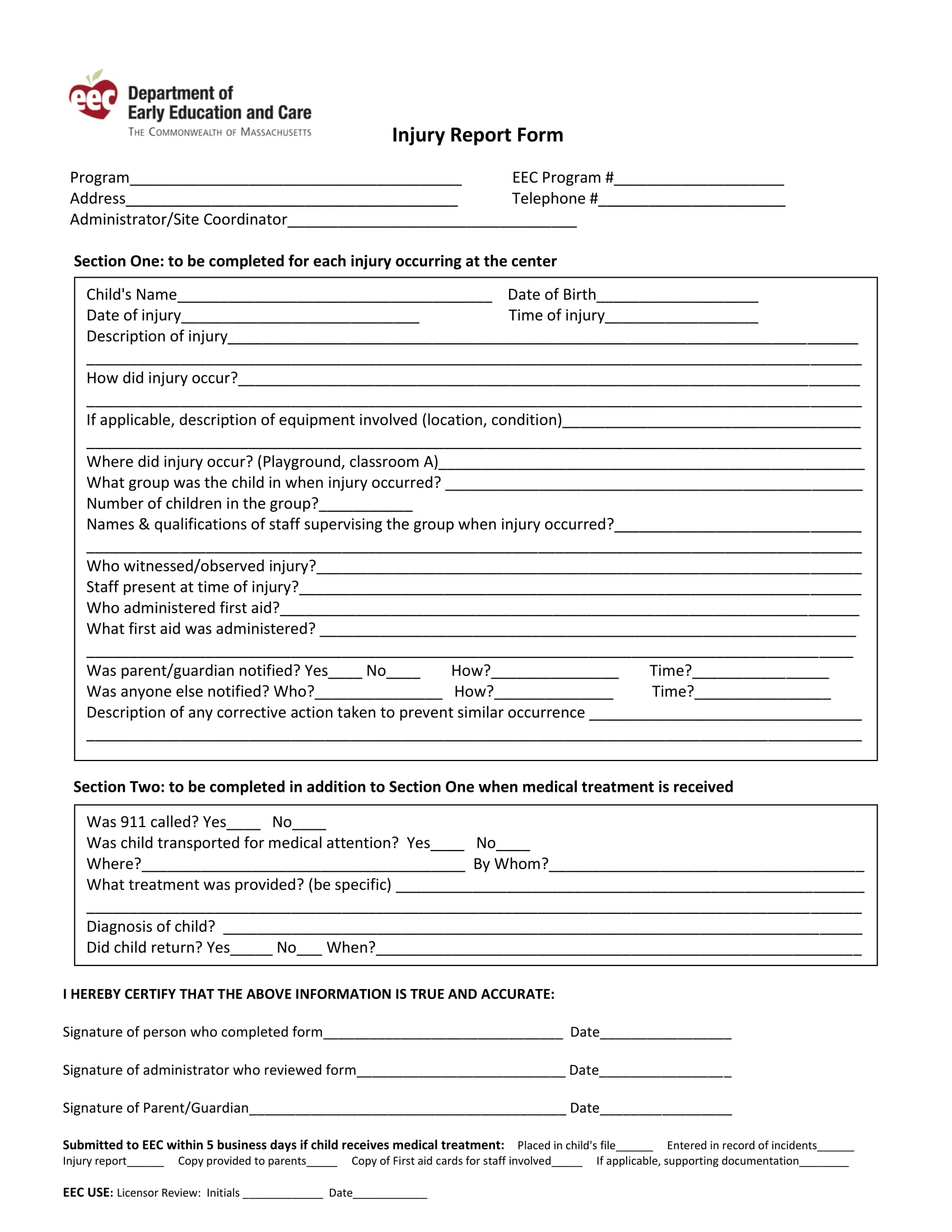
First Report Of Injury Form
First Report Of Injury Form - Your insurer will report the injury to the department of labor and industry (department), when necessary. It should be typed or legibly printed, signed, and dated by the preparer. Web employer's first report of injury. Name (last, first, m.i.) 2. Web employer's first report of injury or disease document number: Part of body injured or exposed* 6. Web this form quickly to allow your insurer time to investigate the claim. This can be done via telephone, facsimile or electronic transmission, to be followed by the froi form within seven days of the occurrence. Web deaths and serious injuries must be reported to the department within 48 hours. This helps us to identify and correct hazards before they cause serious injuries.
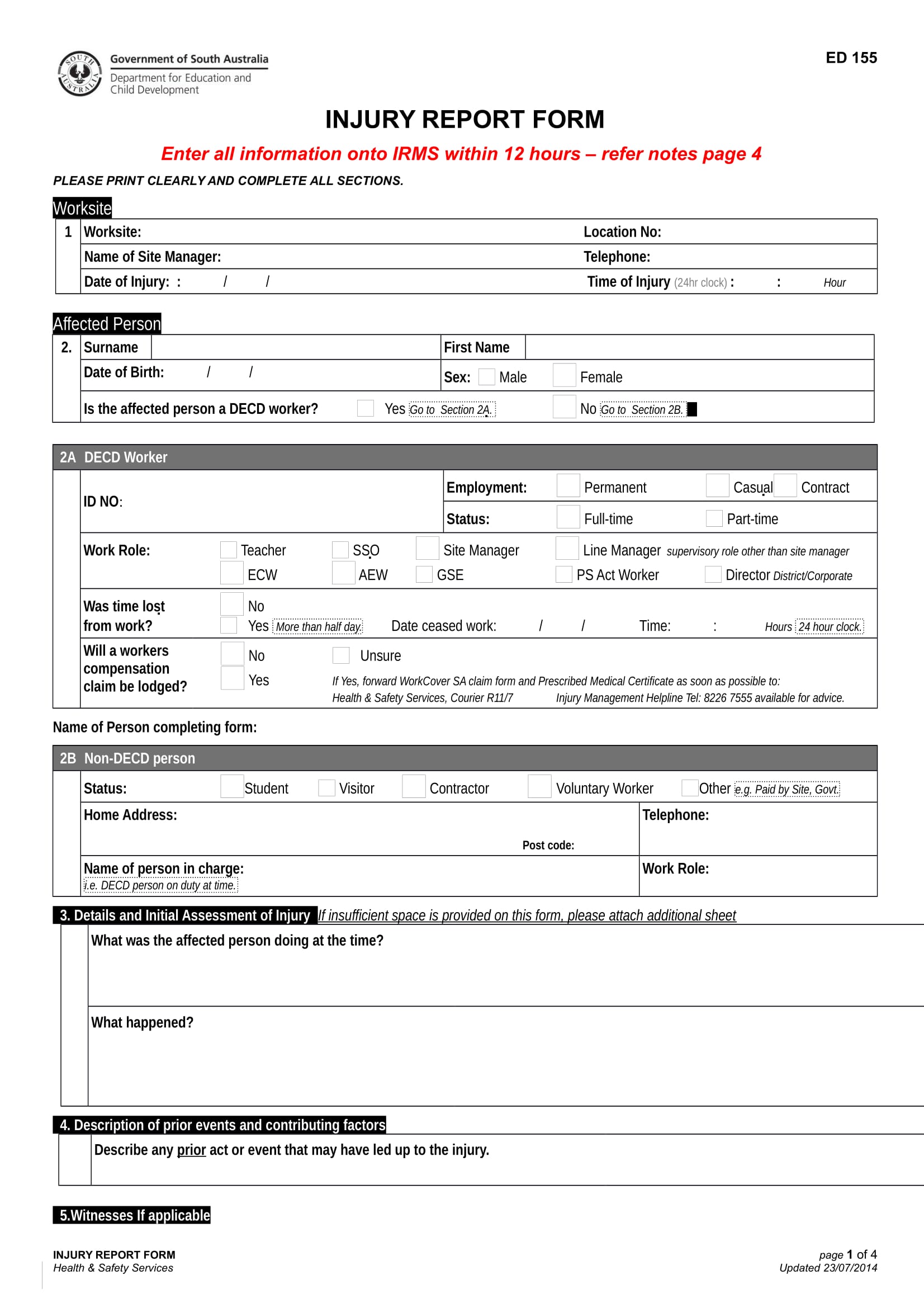
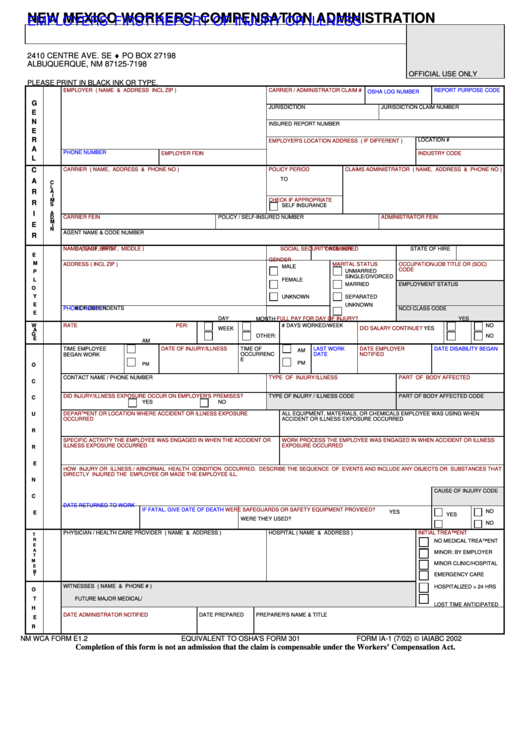
Web describe how the injury or illness/abnormal health condition occurred. You may file your first report of injury (form 101), your monthly payment reports (form 107) and a request for extension of time online using the first report of injury management system. Web first report of injury. Worker stepped to the edge of the scaffolding to inspect work, lost balance and fell six feet to the floor. Web employer's first report of injury or disease document number: Your insurer will report the injury to the department of labor and industry (department), when necessary. Web the use of this form is required under the provisions of the tennessee workers'compensation law and must be completed and filed with your insurance carrier immediately after notice of injury. Include the sequence of events and name any objects or substance that directly injured the employee or made the employee ill. Date and time of accident (mm/dd/yyyy) (hh:mm am/pm) 4. Part of body injured or exposed* 6.
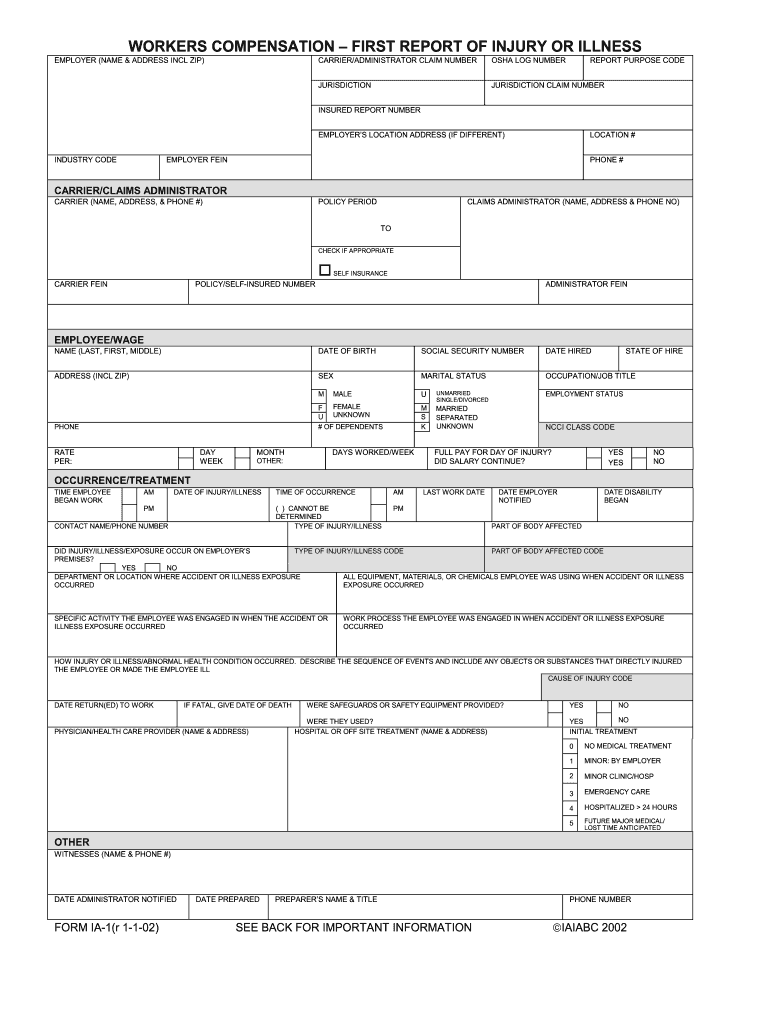
Part of body injured or exposed* 6. Send the original form to the claim administrator for the insurance company who provided insurance coverage on the date of the occurrence. Date and time of accident (mm/dd/yyyy) (hh:mm am/pm) 4. It is a crime to knowingly provide false, incomplete or misleading information to any party to a workers' compensation transaction for the purpose of. This helps us to identify and correct hazards before they cause serious injuries. Does the employee speak english? The employer must also send a. Web employer's first report of injury or disease document number: You may file your first report of injury (form 101), your monthly payment reports (form 107) and a request for extension of time online using the first report of injury management system. Web describe how the injury or illness/abnormal health condition occurred.
FREE 15+ Injury Report Forms in MS Word PDF Excel
Web first report of injury. This helps us to identify and correct hazards before they cause serious injuries. The employer must also send a. Date and time of accident (mm/dd/yyyy) (hh:mm am/pm) 4. Include the sequence of events and name any objects or substance that directly injured the employee or made the employee ill.

Minnesota First Report Of Injury Form PDFSimpli
Web employer's first report of injury. Include the sequence of events and name any objects or substance that directly injured the employee or made the employee ill. Web describe how the injury or illness/abnormal health condition occurred. Web deaths and serious injuries must be reported to the department within 48 hours. It should be typed or legibly printed, signed, and.
FREE 15+ Injury Report Forms in MS Word PDF Excel
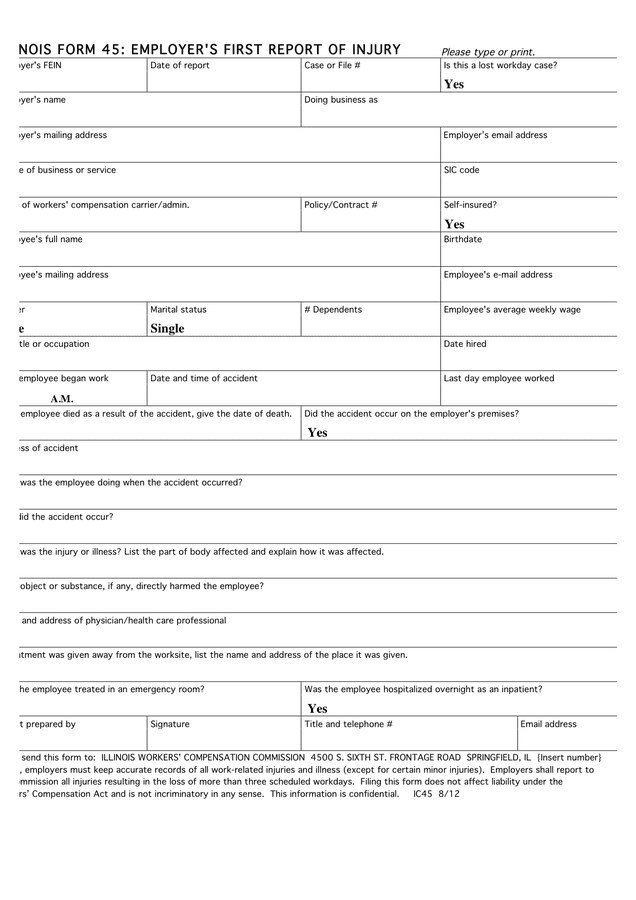
Send the original form to the claim administrator for the insurance company who provided insurance coverage on the date of the occurrence. It is a crime to knowingly provide false, incomplete or misleading information to any party to a workers' compensation transaction for the purpose of. Name (last, first, m.i.) 2. Web employer's first report of injury or disease document.
Employer's first report of injury form in Word and Pdf formats
Send the original form to the claim administrator for the insurance company who provided insurance coverage on the date of the occurrence. The employer must also send a. It is a crime to knowingly provide false, incomplete or misleading information to any party to a workers' compensation transaction for the purpose of. You may file your first report of injury.
Workers Compensation Nj Forms Fill Out and Sign Printable PDF
Home phone ( ) 5. Send the original form to the claim administrator for the insurance company who provided insurance coverage on the date of the occurrence. Web describe how the injury or illness/abnormal health condition occurred. Include the sequence of events and name any objects or substance that directly injured the employee or made the employee ill. Web the.

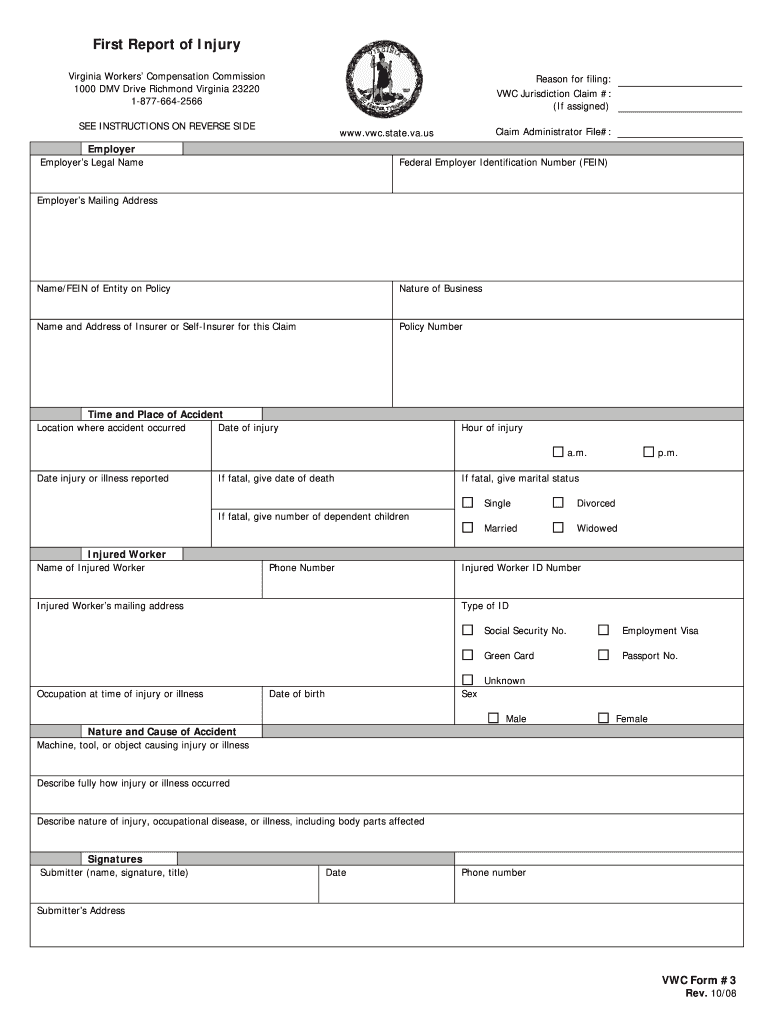
South Carolina First Report of Injury Form from
It should be typed or legibly printed, signed, and dated by the preparer. The employer must also send a. Part of body injured or exposed* 6. Send the original form to the claim administrator for the insurance company who provided insurance coverage on the date of the occurrence. Web describe how the injury or illness/abnormal health condition occurred.
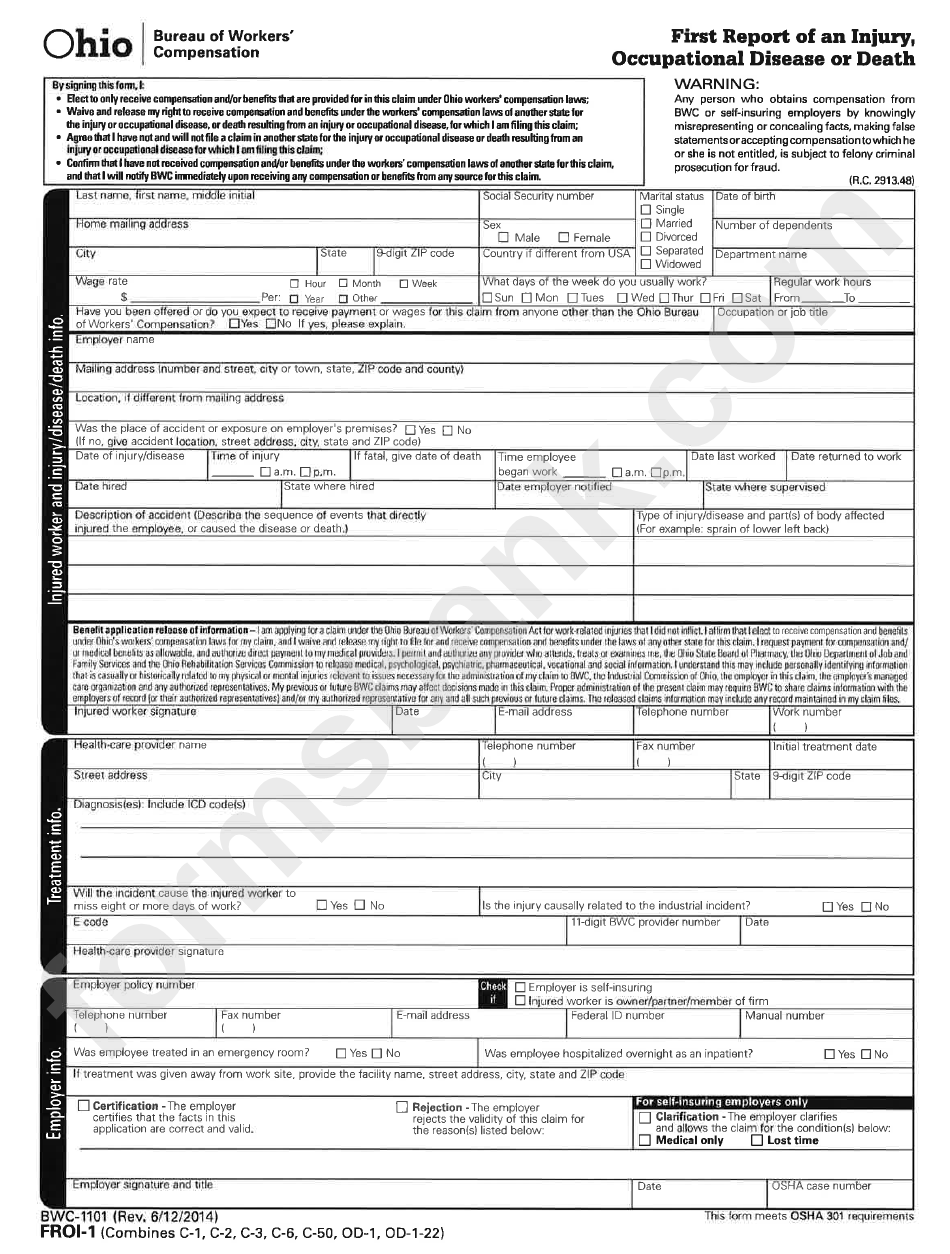
First Report Of Injury Bwc Form Ohio printable pdf download
The employer must also send a. Worker stepped to the edge of the scaffolding to inspect work, lost balance and fell six feet to the floor. Department of labor (see instructions on reverse) office of workers' compensation programs omb no. You may file your first report of injury (form 101), your monthly payment reports (form 107) and a request for.
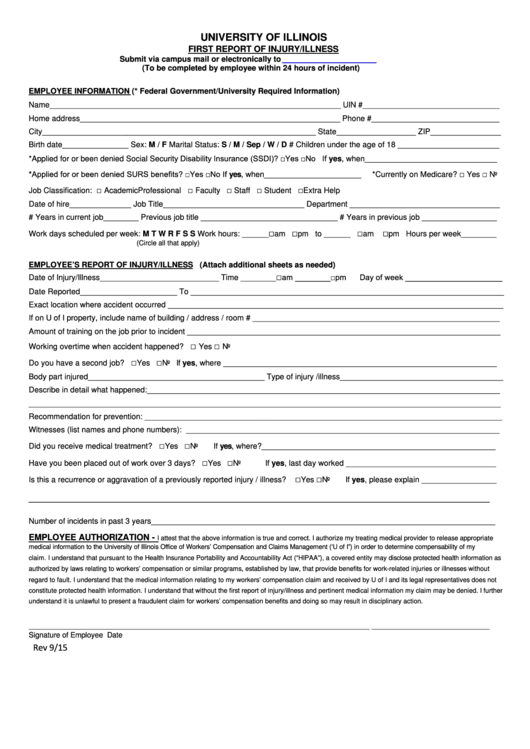
First Report Of Injury/illness Form printable pdf download
You may file your first report of injury (form 101), your monthly payment reports (form 107) and a request for extension of time online using the first report of injury management system. Your insurer will report the injury to the department of labor and industry (department), when necessary. Filing online using the first report of injury management system (for insurance.
Fillable First Report Of Injury printable pdf download
Web employer's first report of injury. This helps us to identify and correct hazards before they cause serious injuries. Web the use of this form is required under the provisions of the tennessee workers'compensation law and must be completed and filed with your insurance carrier immediately after notice of injury. It is a crime to knowingly provide false, incomplete or.
First Injury Report Fill Online, Printable, Fillable, Blank pdfFiller
The employer must also send a. Your insurer will report the injury to the department of labor and industry (department), when necessary. Web deaths and serious injuries must be reported to the department within 48 hours. Department of labor (see instructions on reverse) office of workers' compensation programs omb no. This helps us to identify and correct hazards before they.
Does The Employee Speak English?
Filing online using the first report of injury management system (for insurance companies only) It should be typed or legibly printed, signed, and dated by the preparer. Web first report of injury. Department of labor (see instructions on reverse) office of workers' compensation programs omb no.
Include The Sequence Of Events And Name Any Objects Or Substance That Directly Injured The Employee Or Made The Employee Ill.
Web describe how the injury or illness/abnormal health condition occurred. This can be done via telephone, facsimile or electronic transmission, to be followed by the froi form within seven days of the occurrence. Part of body injured or exposed* 6. It is a crime to knowingly provide false, incomplete or misleading information to any party to a workers' compensation transaction for the purpose of.
Name (Last, First, M.i.) 2.
This helps us to identify and correct hazards before they cause serious injuries. Web deaths and serious injuries must be reported to the department within 48 hours. Web this form quickly to allow your insurer time to investigate the claim. Send the original form to the claim administrator for the insurance company who provided insurance coverage on the date of the occurrence.
You May File Your First Report Of Injury (Form 101), Your Monthly Payment Reports (Form 107) And A Request For Extension Of Time Online Using The First Report Of Injury Management System.
Worker stepped to the edge of the scaffolding to inspect work, lost balance and fell six feet to the floor. Web the use of this form is required under the provisions of the tennessee workers'compensation law and must be completed and filed with your insurance carrier immediately after notice of injury. Web employer's first report of injury or disease document number: Date and time of accident (mm/dd/yyyy) (hh:mm am/pm) 4.