Doh 4359 Form Pdf
Doh 4359 Form Pdf - Hiv/aids educational materials order forms. Easily fill out pdf blank, edit, and sign them. Expanded syringe access program (esap) forms. Customize your document by using the toolbar on the top. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Download your finished form and share it as you needed. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Patient identifying information (use additional paper if necessary) 2. Save or instantly send your ready documents. Wait until doh 4359 form is ready.
Easily fill out pdf blank, edit, and sign them. Patient identifying information (use additional paper if necessary) 2. The best place to get access to and use this form is here. For the condition(s) requiring personal care: Download your finished form and share it as you needed. Expanded syringe access program (esap) forms. It is a form issued by the department of health in a particular jurisdiction, and the content and purpose of the form can vary depending on the specific jurisdiction. Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery. Save or instantly send your ready documents. To start with, look for the “get form” button and tap it.
• primary and secondary diagnosis. Web read the following instructions to use cocodoc to start editing and filling out your doh 4359 form: To start with, look for the “get form” button and tap it. Hiv/aids educational materials order forms. Customize your document by using the toolbar on the top. Web the doh 4359 form is a printable document that is used for various purposes related to healthcare. We are not affiliated with any brand or entity on this form. Wait until doh 4359 form is ready. It is a form issued by the department of health in a particular jurisdiction, and the content and purpose of the form can vary depending on the specific jurisdiction. Easily fill out pdf blank, edit, and sign them.

Doh 4359 form Fill out & sign online DocHub
Download your finished form and share it as you needed. Wait until doh 4359 form is ready. Patient identifying information (use additional paper if necessary) 2. Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery. Web the doh 4359 form is a printable document.
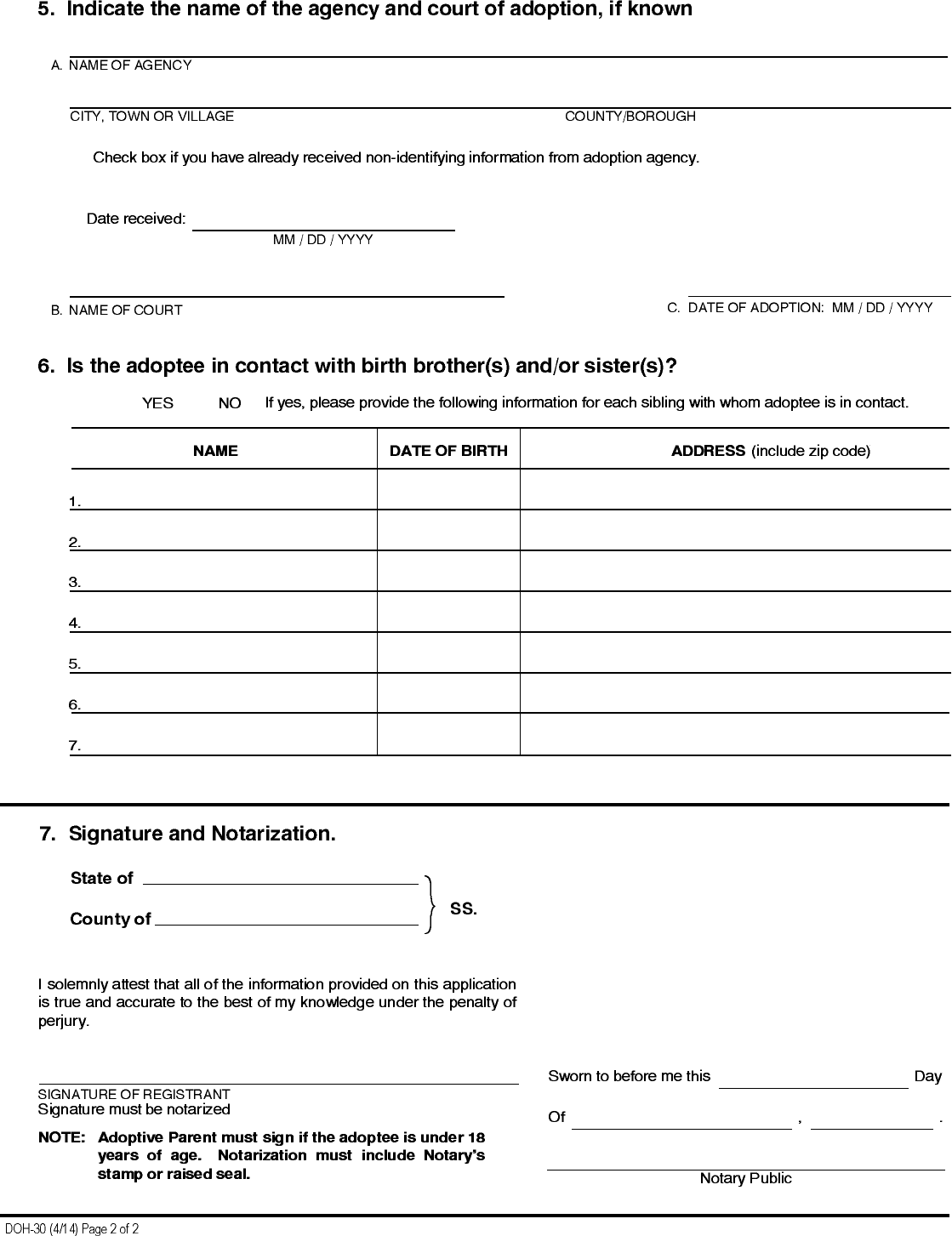
Form Doh30 Adoptee Registration Form Edit, Fill, Sign Online
Hiv/aids educational materials order forms. Patient identifying information (use additional paper if necessary) 2. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Patient identifying information (use additional paper if necessary) 2. Download your finished form and share it as you needed.
Doh 4359 Form ≡ Fill Out Printable PDF Forms Online
The best place to get access to and use this form is here. Save or instantly send your ready documents. Easily fill out pdf blank, edit, and sign them. Patient identifying information (use additional paper if necessary) 2. Web the doh 4359 form is a printable document that is used for various purposes related to healthcare.
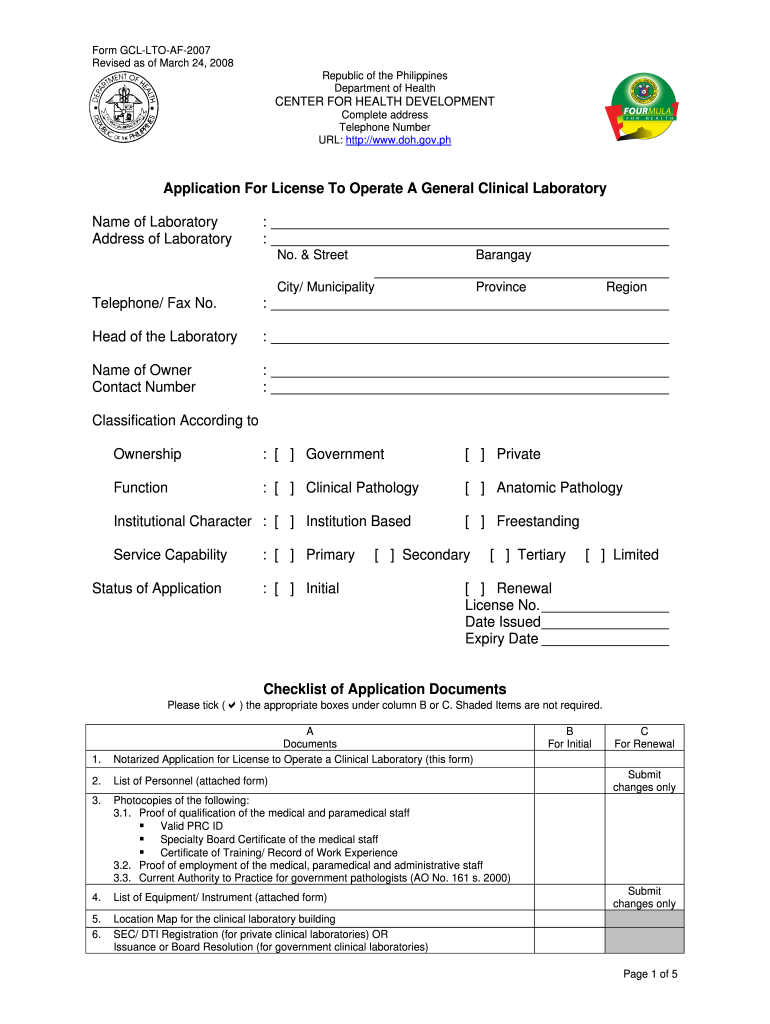
Doh Application Form for Renewal of License to Operate Fill Out and
For the condition(s) requiring personal care: Download your finished form and share it as you needed. Save or instantly send your ready documents. Enter the patient’s height and weight. Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery.

Form DOH4359 Download Fillable PDF or Fill Online Physician's Order
Patient identifying information (use additional paper if necessary) 2. Web read the following instructions to use cocodoc to start editing and filling out your doh 4359 form: It is a form issued by the department of health in a particular jurisdiction, and the content and purpose of the form can vary depending on the specific jurisdiction. Web the doh 4359.

Doh 4402 Form Fill Online, Printable, Fillable, Blank pdfFiller
Save or instantly send your ready documents. Get the doh 4359 2010 template, fill it out, esign it, and share it in minutes. Web read the following instructions to use cocodoc to start editing and filling out your doh 4359 form: Easily fill out pdf blank, edit, and sign them. Patient identifying information (use additional paper if necessary) 2.
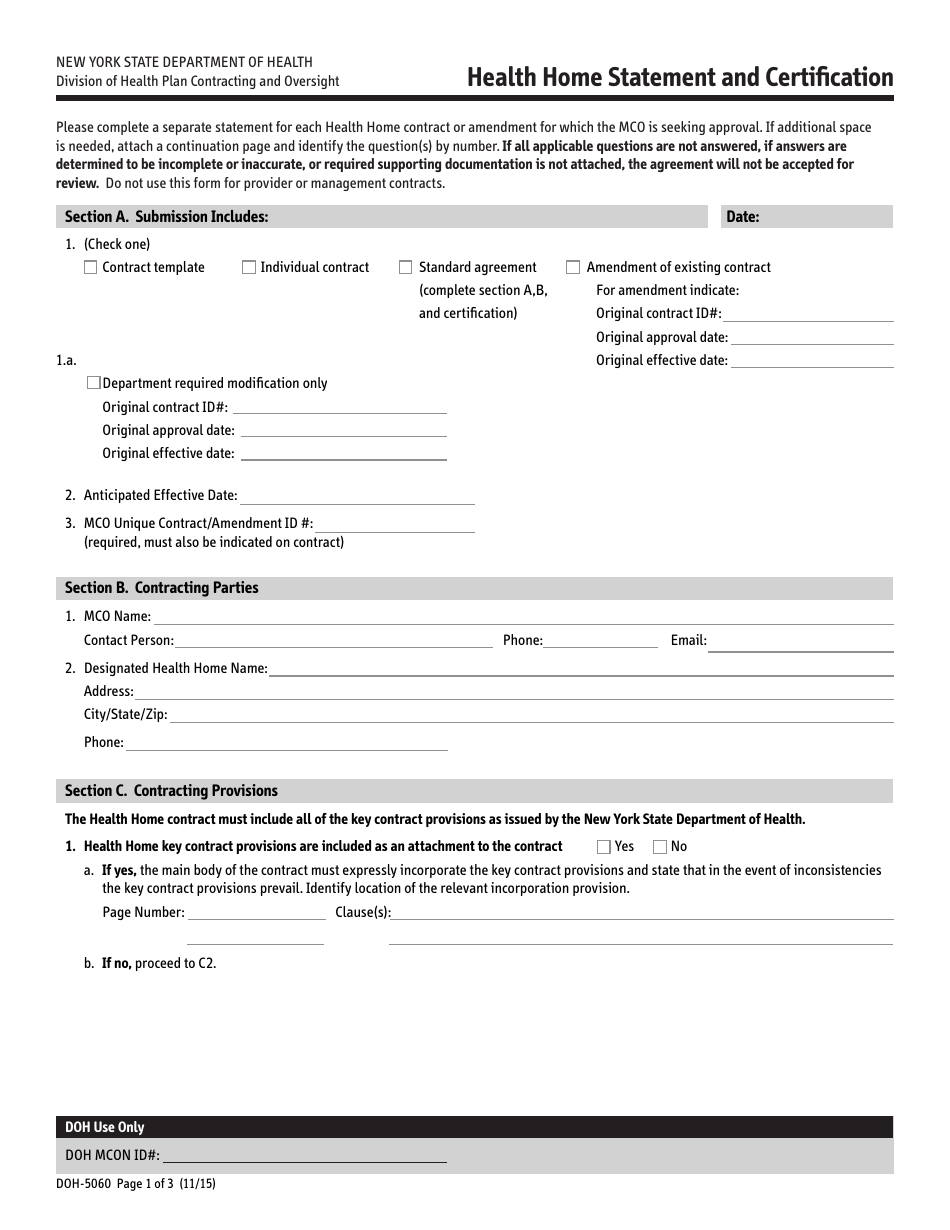
Form DOH5060 Download Printable PDF or Fill Online Health Home
The best place to get access to and use this form is here. • primary and secondary diagnosis. To start with, look for the “get form” button and tap it. Web read the following instructions to use cocodoc to start editing and filling out your doh 4359 form: Web the doh 4359 form is a form that all hospitals must.
Form DOH4181 Download Printable PDF or Fill Online Adoption
Web the doh 4359 form is a printable document that is used for various purposes related to healthcare. Save or instantly send your ready documents. Hiv/aids educational materials order forms. Web read the following instructions to use cocodoc to start editing and filling out your doh 4359 form: Wait until doh 4359 form is ready.
Form DOH4358 Download Printable PDF or Fill Online Notification From
Hiv/aids educational materials order forms. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Easily fill out pdf blank,.
Download da 4359 Fillable Form
Hiv/aids educational materials order forms. To start with, look for the “get form” button and tap it. Wait until doh 4359 form is ready. It is a form issued by the department of health in a particular jurisdiction, and the content and purpose of the form can vary depending on the specific jurisdiction. Expanded syringe access program (esap) forms.
Wait Until Doh 4359 Form Is Ready.
Patient identifying information (use additional paper if necessary) 2. Web the doh 4359 form is a form that all hospitals must submit to the department of health, detailing deaths and serious injuries during surgery. To start with, look for the “get form” button and tap it. We are not affiliated with any brand or entity on this form.
Get The Doh 4359 2010 Template, Fill It Out, Esign It, And Share It In Minutes.
It is a form issued by the department of health in a particular jurisdiction, and the content and purpose of the form can vary depending on the specific jurisdiction. The best place to get access to and use this form is here. Hiv/aids educational materials order forms. Customize your document by using the toolbar on the top.
Expanded Syringe Access Program (Esap) Forms.
Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. • primary and secondary diagnosis. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Easily fill out pdf blank, edit, and sign them.
For The Condition(S) Requiring Personal Care:
Download your finished form and share it as you needed. Indicate n/a if an item does not apply to this patient or unk if the requested information is unknown to the physician signing this form. Patient identifying information (use additional paper if necessary) 2. Enter the patient’s height and weight.