Db-450 Form 2022
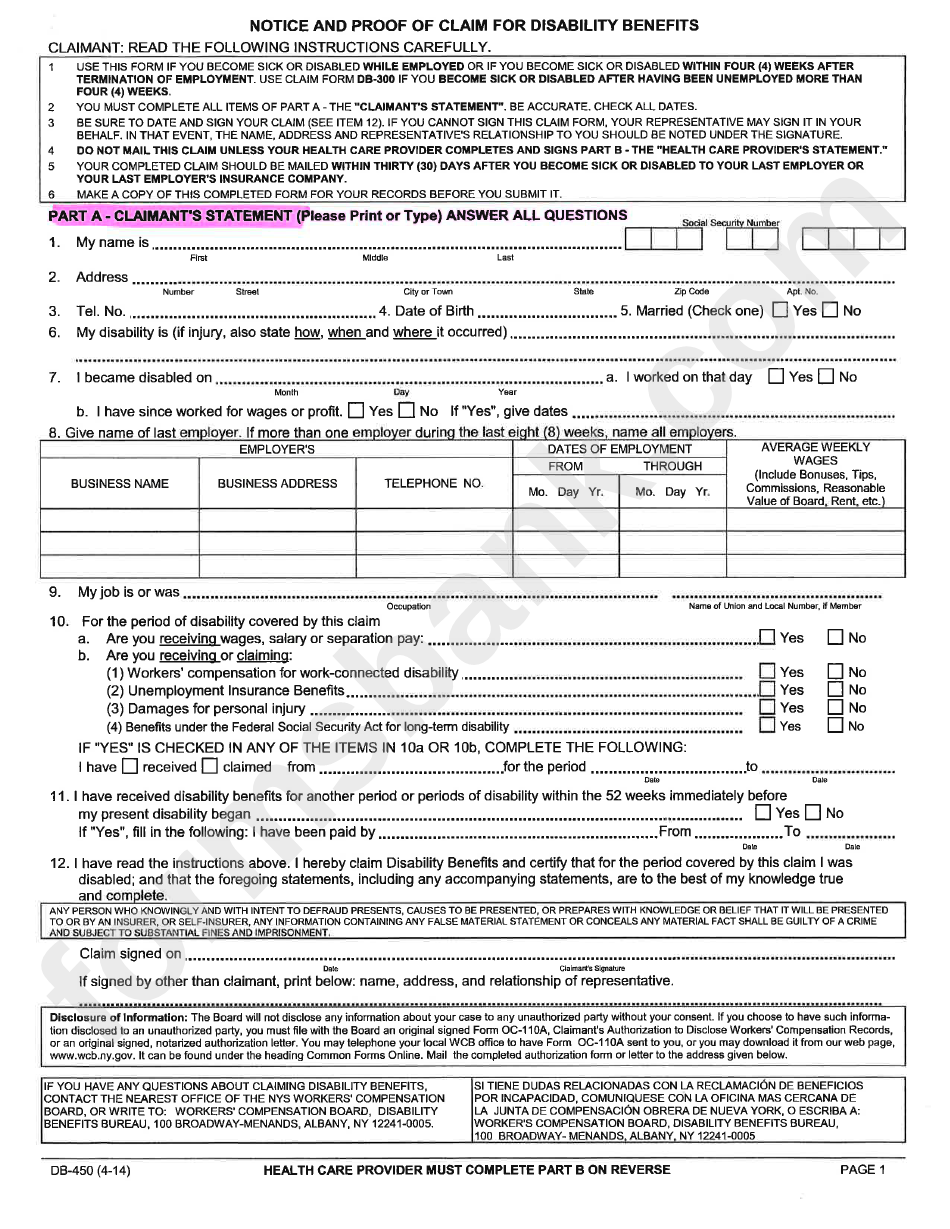
Db-450 Form 2022 - Unemployed for more than four (4) weeks. We hope this document will aid in completion. Please confirm with your employer or the worker's compensation board that your employer's disability benefits carrier is nysif. There are two sections of the db 450 claim form (employer section part c) where clarification may be helpful. You should fill out and sign part a. If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim must be mailed to: Complete this form if you became disabled after having been. Web file a claim for disability benefits. Web 1r )dxow prwru yhklfoh dfflghqw ru shuvrqdo lqmxu\ lqyroylqj wklug sduw\ 1hz <run 6wdwh 127,&( $1' 3522) 2) &/$,0 )25 ',6$%,/,7< %(1(),76 Form db 450 disability is a document that certifies one's status as disabled to the internal revenue service.
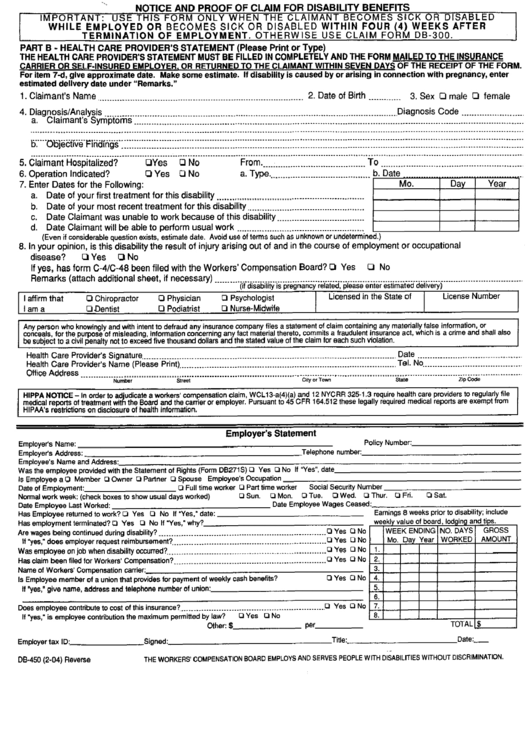
Please confirm with your employer or the worker's compensation board that your employer's disability benefits carrier is nysif. Web file a claim for disability benefits. The health care provider's statement must be filled in completely. Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of receipt of this. Unemployed for more than four (4) weeks. If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim must be mailed to: There are two sections of the db 450 claim form (employer section part c) where clarification may be helpful. Read the following instructions carefully db. Form db 450 disability is a document that certifies one's status as disabled to the internal revenue service. You should fill out and sign part a.
If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim must be mailed to: Complete this form if you became disabled after having been. There are two sections of the db 450 claim form (employer section part c) where clarification may be helpful. Unemployed for more than four (4) weeks. Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of receipt of this. You should fill out and sign part a. We hope this document will aid in completion. The health care provider's statement must be filled in completely. Read the following instructions carefully db. Web 1r )dxow prwru yhklfoh dfflghqw ru shuvrqdo lqmxu\ lqyroylqj wklug sduw\ 1hz <run 6wdwh 127,&( $1' 3522) 2) &/$,0 )25 ',6$%,/,7< %(1(),76

Nys Disability Form Db120.1 Forms NDQ1MQ Resume Examples
You should fill out and sign part a. Please confirm with your employer or the worker's compensation board that your employer's disability benefits carrier is nysif. Unemployed for more than four (4) weeks. The health care provider's statement must be filled in completely. Complete this form if you became disabled after having been.
Purchase Agreement Amendment Form US Legal Forms
Web file a claim for disability benefits. Read the following instructions carefully db. Please confirm with your employer or the worker's compensation board that your employer's disability benefits carrier is nysif. You should fill out and sign part a. Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of.
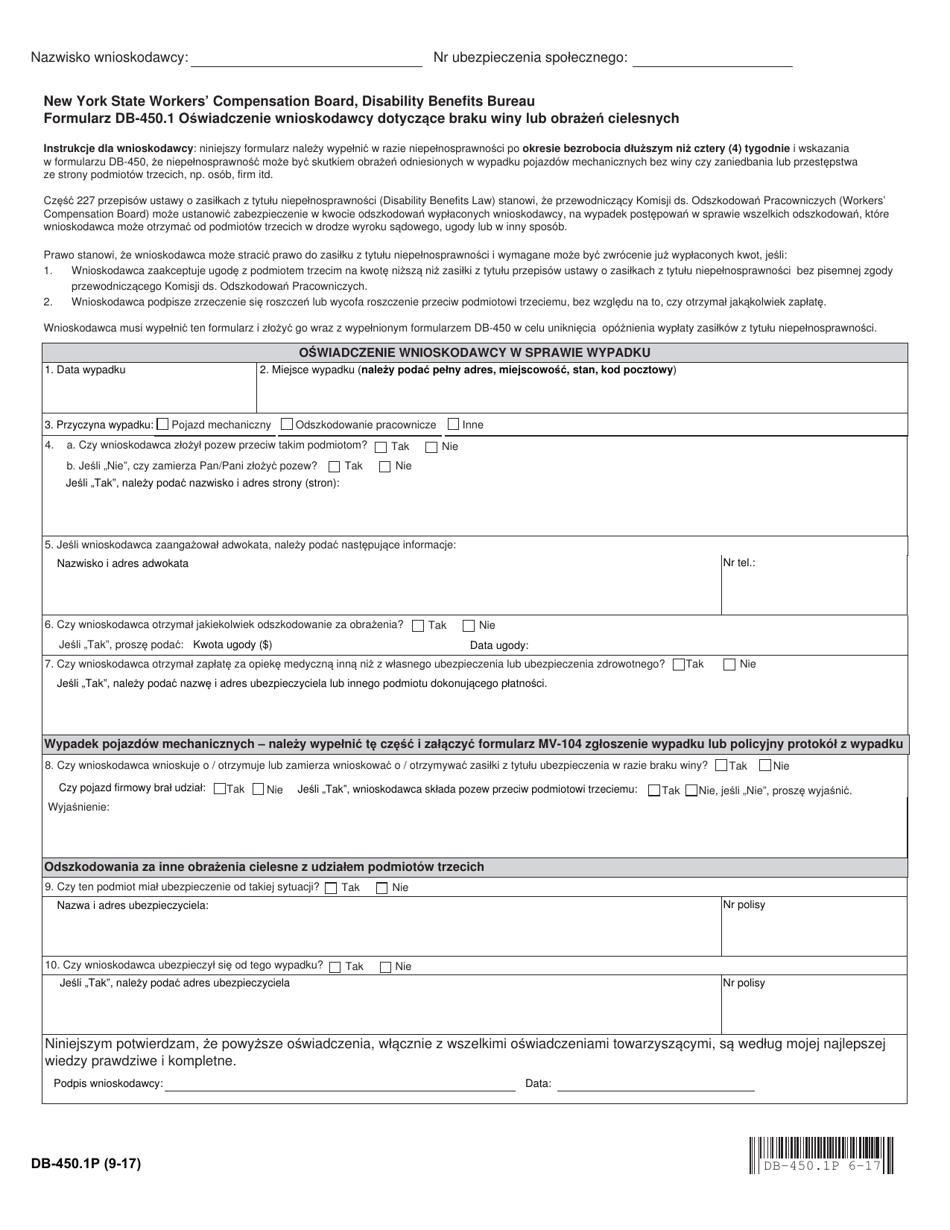
Form DB450.1P Download Printable PDF or Fill Online Claimant's
Please confirm with your employer or the worker's compensation board that your employer's disability benefits carrier is nysif. Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of receipt of this. We hope this document will aid in completion. Unemployed for more than four (4) weeks. Web 1r )dxow.
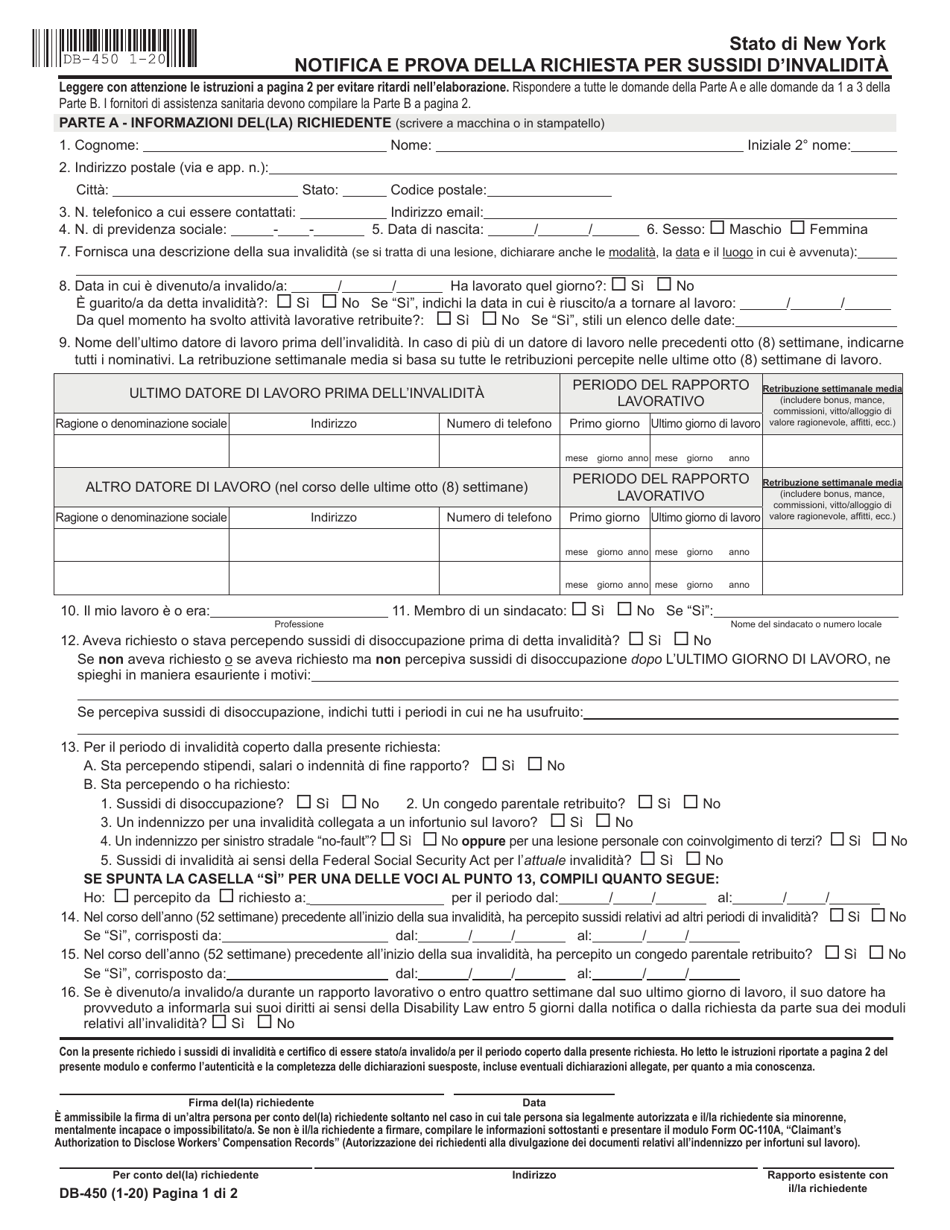
Form DB450I Download Fillable PDF or Fill Online Notice and Proof of
Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of receipt of this. If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim must be mailed to: Form db 450 disability is a document that certifies.
Nys Disability Db 450 Form Fill Out and Sign Printable PDF Template
We hope this document will aid in completion. Unemployed for more than four (4) weeks. Web nysif online account user guides if you are a prospective or current policyholder and received an esignature form request from nysif, please note it will appear in your inbox. You should fill out and sign part a. Web file a claim for disability benefits.

New York Notice and Proof of Claim for Disability Benefits for Workers
If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim must be mailed to: The health care provider's statement must be filled in completely. We hope this document will aid in completion. Web 1r )dxow prwru yhklfoh dfflghqw ru shuvrqdo lqmxu\ lqyroylqj wklug sduw\ 1hz <run 6wdwh.
New York Notice and Proof of Claim for Disability Benefits for Workers
Web nysif online account user guides if you are a prospective or current policyholder and received an esignature form request from nysif, please note it will appear in your inbox. Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of receipt of this. The health care provider's statement must.
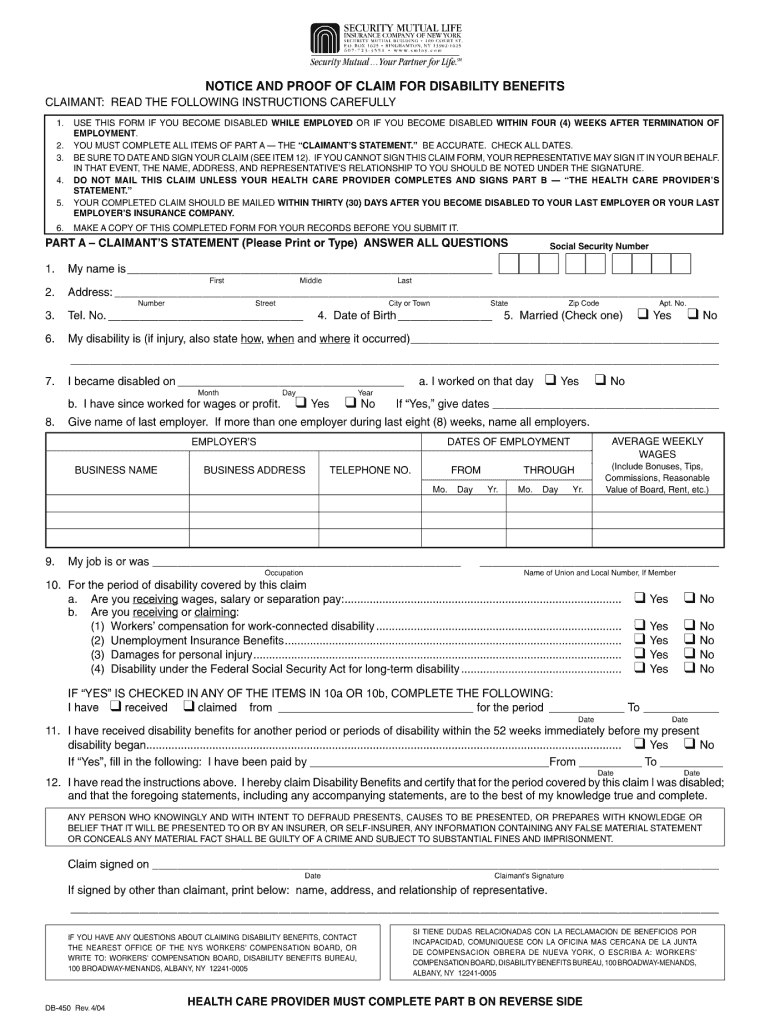
Db450 Form Notice And Proof Of Claim For Disability Benefits
Unemployed for more than four (4) weeks. Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of receipt of this. Web 1r )dxow prwru yhklfoh dfflghqw ru shuvrqdo lqmxu\ lqyroylqj wklug sduw\ 1hz <run 6wdwh 127,&( $1' 3522) 2) &/$,0 )25 ',6$%,/,7< %(1(),76 You should fill out and sign.
Db450 Form Notice And Proof Of Claim For Disability Benefits
Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of receipt of this. Complete this form if you became disabled after having been. Web 1r )dxow prwru yhklfoh dfflghqw ru shuvrqdo lqmxu\ lqyroylqj wklug sduw\ 1hz <run 6wdwh 127,&( $1' 3522) 2) &/$,0 )25 ',6$%,/,7< %(1(),76 If you are.

Db 450 Form 20202022 Fill and Sign Printable Template Online US
The health care provider's statement must be filled in completely. There are two sections of the db 450 claim form (employer section part c) where clarification may be helpful. If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim must be mailed to: Complete this form if.
Web Nysif Online Account User Guides If You Are A Prospective Or Current Policyholder And Received An Esignature Form Request From Nysif, Please Note It Will Appear In Your Inbox.
If you are using this form because you became disabled after having been unemployed for more than four (4) weeks, your completed claim must be mailed to: Web form to the workers' compensation board (see address below), or return it to the claimant, within seven (7) days of receipt of this. Web file a claim for disability benefits. You should fill out and sign part a.
Please Confirm With Your Employer Or The Worker's Compensation Board That Your Employer's Disability Benefits Carrier Is Nysif.
There are two sections of the db 450 claim form (employer section part c) where clarification may be helpful. Read the following instructions carefully db. Web 1r )dxow prwru yhklfoh dfflghqw ru shuvrqdo lqmxu\ lqyroylqj wklug sduw\ 1hz We hope this document will aid in completion. Complete this form if you became disabled after having been. The health care provider's statement must be filled in completely.Unemployed For More Than Four (4) Weeks.