Certified Payroll Form Wh 347
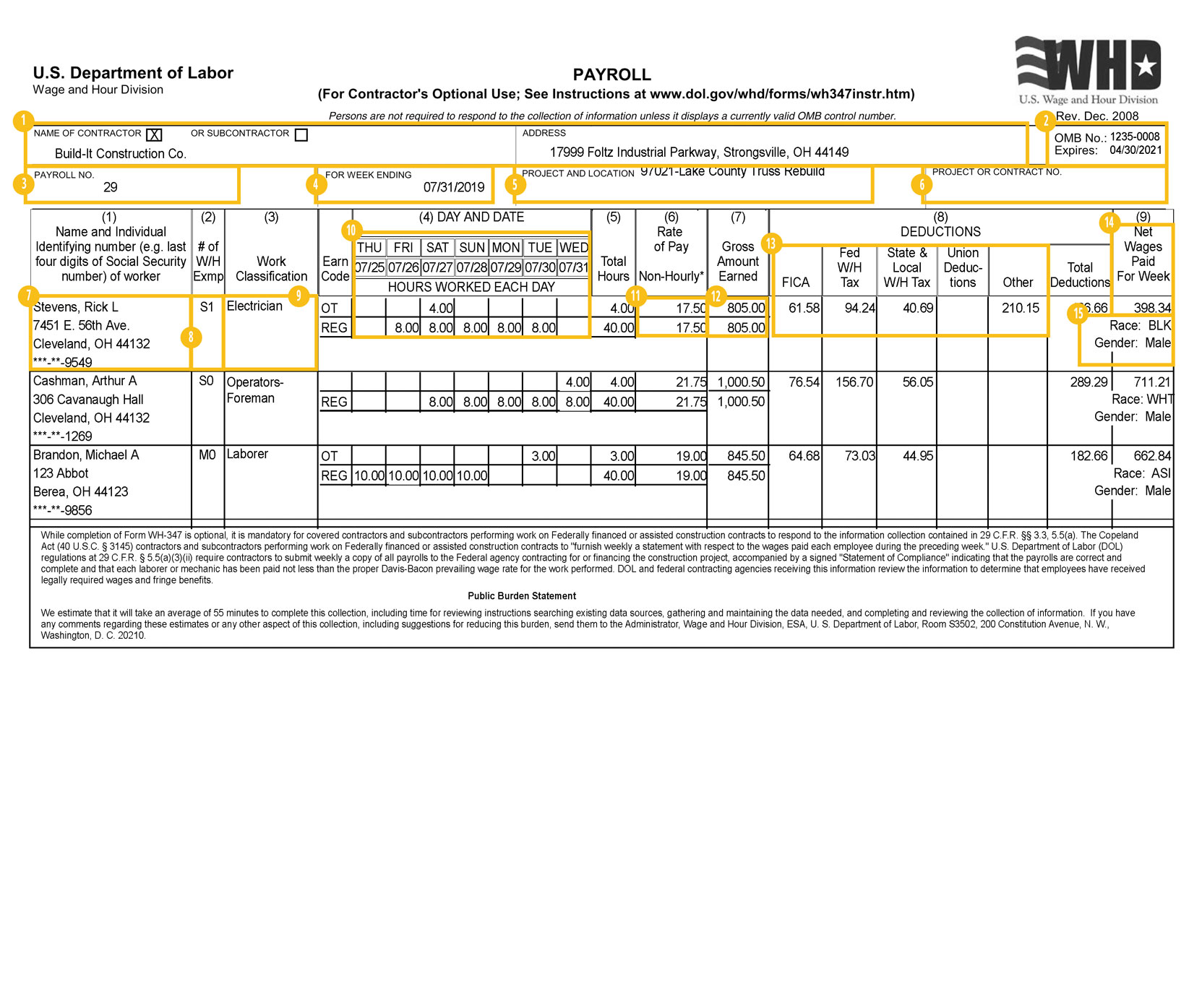
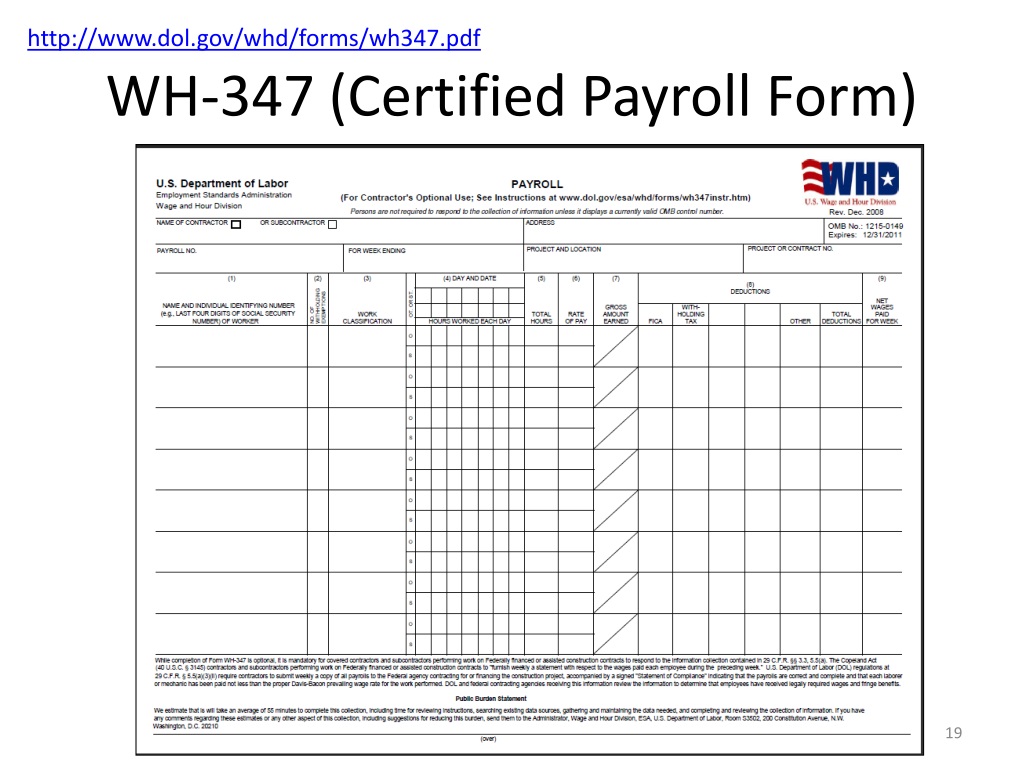
Certified Payroll Form Wh 347 - Fmla certification of health care provider for employee’s serious health condition. List the workweek ending date. Fill in your firm's address. Fill in your firm's name and check appropriate box. The form is broken down into two files pdf and instructions. You’ll need to enter some basic payroll data on the form, including each worker’s name, social security number, and tax withholding information. Fillfill outout completelycompletely withwith contractorcontractor oror thethe lastlast dayday ofof thethe subcontractorsubcontractor addressaddresscheckcheck oneone ofof thethe boxesboxes andandpayrollpayroll period.period. Beginning with the number 1, list the payroll number for the submission. Dot is committed to ensuring that information is available in appropriate alternative formats to meet the requirements of persons who have a disability. Sf 308 request for wage determination and response to request.
If you require an alternative version of files provided on this page, please contact flh.webmaster@dot.gov. Beginning with the number 1, list the payroll number for the submission. You’ll need to enter some basic payroll data on the form, including each worker’s name, social security number, and tax withholding information. If you need a little help to with the. Sf 308 request for wage determination and response to request. Web • weekly payrolls must include specific information as required by 29 c.f.r. Fillfill outout completelycompletely withwith contractorcontractor oror thethe lastlast dayday ofof thethe subcontractorsubcontractor addressaddresscheckcheck oneone ofof thethe boxesboxes andandpayrollpayroll period.period. List the workweek ending date. The form is broken down into two files pdf and instructions. Fill in your firm's name and check appropriate box.
Web • weekly payrolls must include specific information as required by 29 c.f.r. Sf 308 request for wage determination and response to request. Fillfill outout completelycompletely withwith contractorcontractor oror thethe lastlast dayday ofof thethe subcontractorsubcontractor addressaddresscheckcheck oneone ofof thethe boxesboxes andandpayrollpayroll period.period. Fill in your firm's name and check appropriate box. The form is broken down into two files pdf and instructions. If you need a little help to with the. If you require an alternative version of files provided on this page, please contact flh.webmaster@dot.gov. Fill in your firm's address. List the workweek ending date. Dot is committed to ensuring that information is available in appropriate alternative formats to meet the requirements of persons who have a disability.

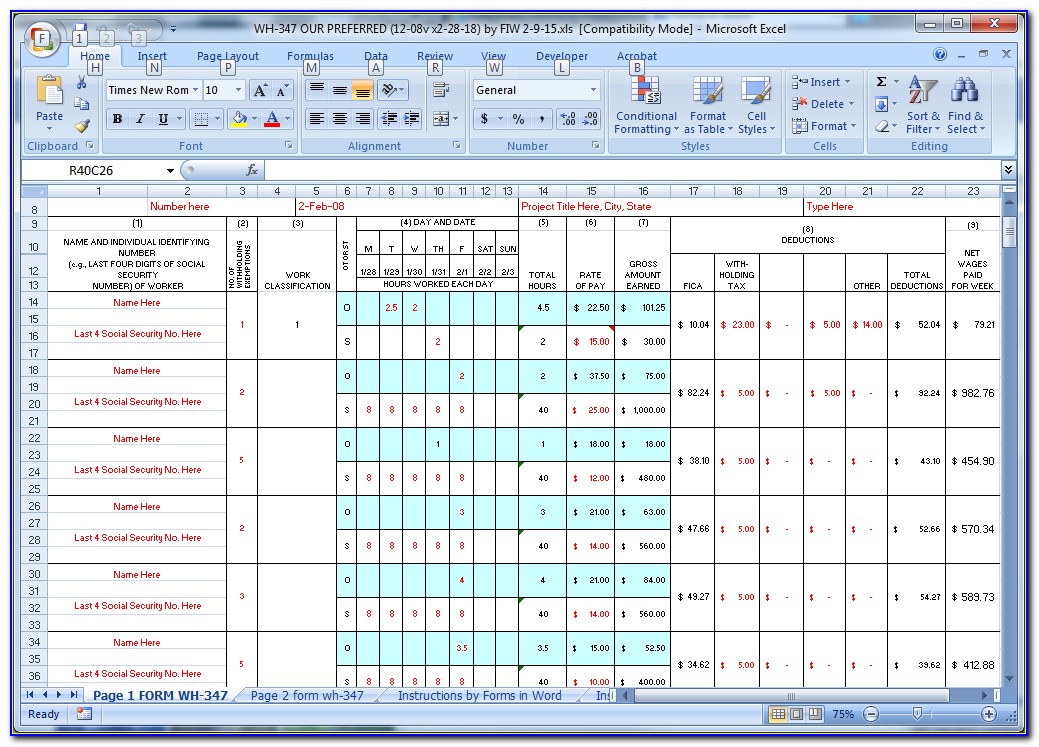
How to fill out certified payroll report Form WH347 eBacon
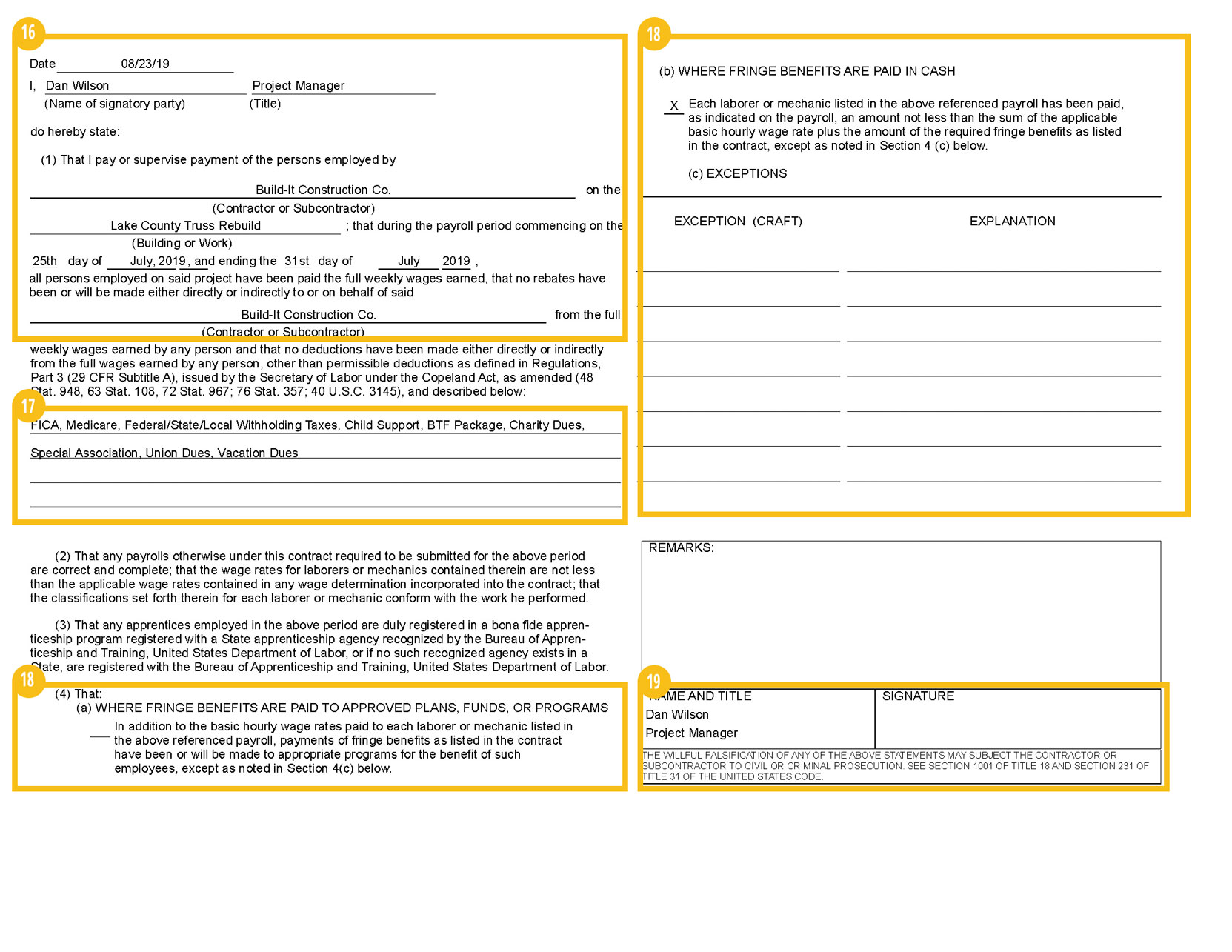
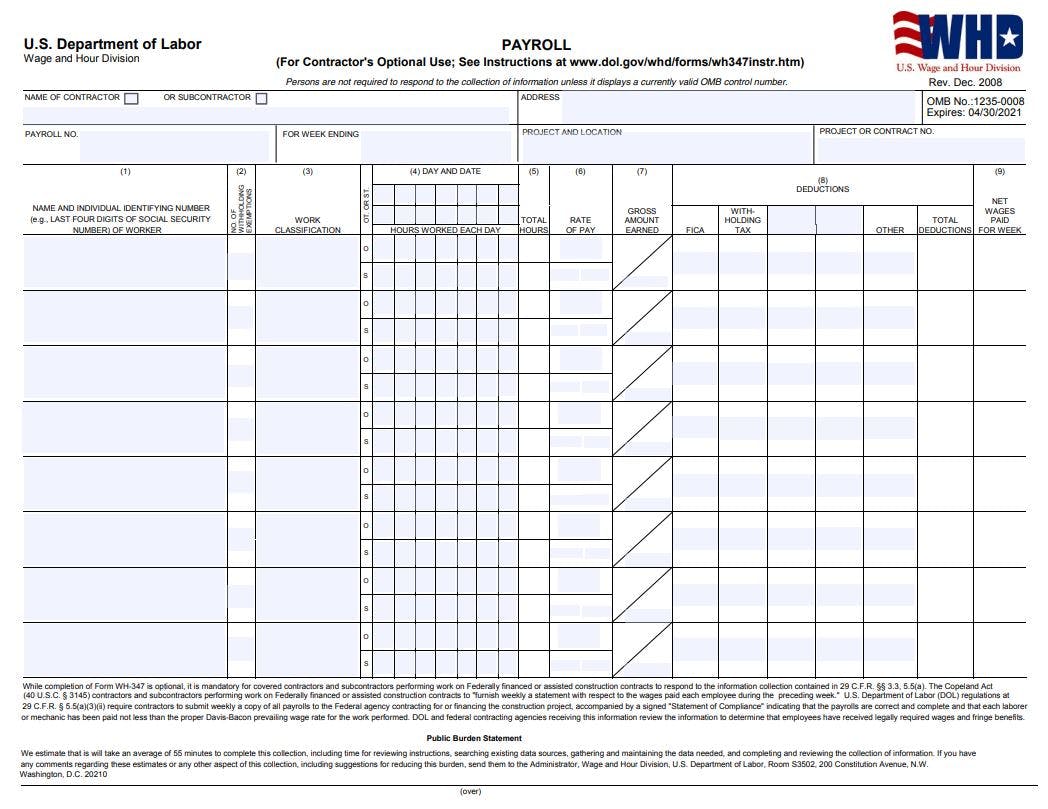
Web detailed instructions concerning the preparation of the payroll follow: Web • weekly payrolls must include specific information as required by 29 c.f.r. If you need a little help to with the. Fillfill outout completelycompletely withwith contractorcontractor oror thethe lastlast dayday ofof thethe subcontractorsubcontractor addressaddresscheckcheck oneone ofof thethe boxesboxes andandpayrollpayroll period.period. Fill in your firm's address.
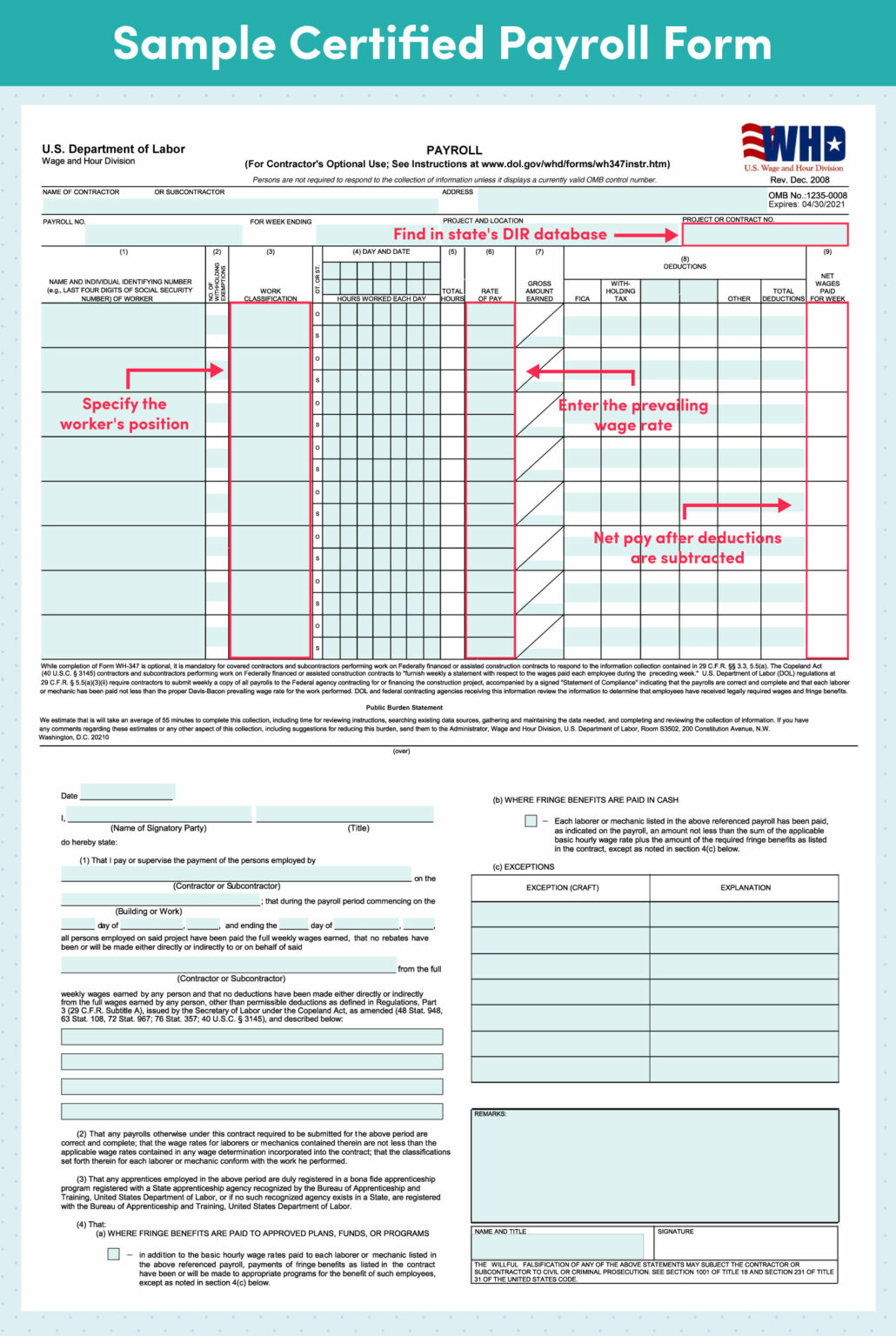
Sample Certified Payroll Report Interact With an Example WH347
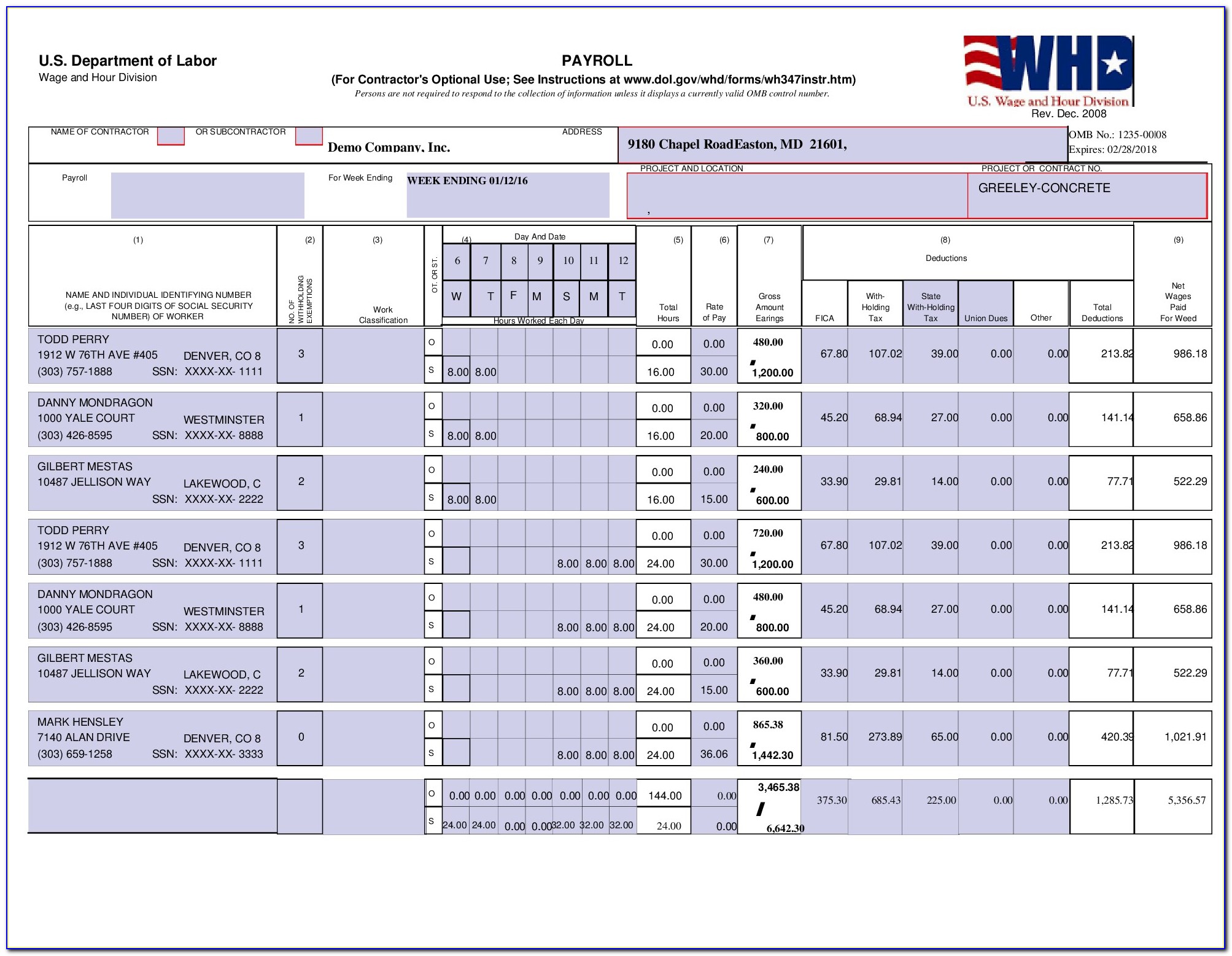
Sf 308 request for wage determination and response to request. You’ll need to enter some basic payroll data on the form, including each worker’s name, social security number, and tax withholding information. Fillfill outout completelycompletely withwith contractorcontractor oror thethe lastlast dayday ofof thethe subcontractorsubcontractor addressaddresscheckcheck oneone ofof thethe boxesboxes andandpayrollpayroll period.period. If you require an alternative version of files provided.
Prevailing Wage Log To Payroll Xls Workbook / Certified Payroll Form Wh
Fill in your firm's address. Web detailed instructions concerning the preparation of the payroll follow: If you need a little help to with the. List the workweek ending date. Sf 308 request for wage determination and response to request.
Sample Certified Payroll Report Interact With an Example WH347
The form is broken down into two files pdf and instructions. Fill in your firm's address. Dot is committed to ensuring that information is available in appropriate alternative formats to meet the requirements of persons who have a disability. Sf 308 request for wage determination and response to request. Fillfill outout completelycompletely withwith contractorcontractor oror thethe lastlast dayday ofof thethe.
Excel format WH347 and WH348 Certified Payroll Form
Web • weekly payrolls must include specific information as required by 29 c.f.r. Beginning with the number 1, list the payroll number for the submission. Fill in your firm's name and check appropriate box. Fmla certification of health care provider for employee’s serious health condition. The form is broken down into two files pdf and instructions.
PPT DavisBacon, Related Acts, and Your Project PowerPoint
Fill in your firm's name and check appropriate box. Sf 308 request for wage determination and response to request. List the workweek ending date. If you need a little help to with the. You’ll need to enter some basic payroll data on the form, including each worker’s name, social security number, and tax withholding information.

Certified Payroll Form Wh 347 Free Form Resume Examples gq965XP2OR
Beginning with the number 1, list the payroll number for the submission. Dot is committed to ensuring that information is available in appropriate alternative formats to meet the requirements of persons who have a disability. If you require an alternative version of files provided on this page, please contact flh.webmaster@dot.gov. Fill in your firm's address. If you need a little.
Certified Payroll Form Wh 347 Instructions Form Resume Examples
Web detailed instructions concerning the preparation of the payroll follow: You’ll need to enter some basic payroll data on the form, including each worker’s name, social security number, and tax withholding information. If you require an alternative version of files provided on this page, please contact flh.webmaster@dot.gov. Sf 308 request for wage determination and response to request. Fill in your.
Certified Payroll for Construction A Complete Guide
You’ll need to enter some basic payroll data on the form, including each worker’s name, social security number, and tax withholding information. Fill in your firm's name and check appropriate box. The form is broken down into two files pdf and instructions. Dot is committed to ensuring that information is available in appropriate alternative formats to meet the requirements of.
Certified Payroll What It Is & How to Report It FinancePal
Web • weekly payrolls must include specific information as required by 29 c.f.r. Fillfill outout completelycompletely withwith contractorcontractor oror thethe lastlast dayday ofof thethe subcontractorsubcontractor addressaddresscheckcheck oneone ofof thethe boxesboxes andandpayrollpayroll period.period. You’ll need to enter some basic payroll data on the form, including each worker’s name, social security number, and tax withholding information. If you require an alternative version.
Web Detailed Instructions Concerning The Preparation Of The Payroll Follow:
Fill in your firm's name and check appropriate box. Fill in your firm's address. Dot is committed to ensuring that information is available in appropriate alternative formats to meet the requirements of persons who have a disability. Beginning with the number 1, list the payroll number for the submission.
Sf 308 Request For Wage Determination And Response To Request.
List the workweek ending date. Fillfill outout completelycompletely withwith contractorcontractor oror thethe lastlast dayday ofof thethe subcontractorsubcontractor addressaddresscheckcheck oneone ofof thethe boxesboxes andandpayrollpayroll period.period. If you need a little help to with the. You’ll need to enter some basic payroll data on the form, including each worker’s name, social security number, and tax withholding information.
Fmla Certification Of Health Care Provider For Employee’s Serious Health Condition.
The form is broken down into two files pdf and instructions. Web • weekly payrolls must include specific information as required by 29 c.f.r. If you require an alternative version of files provided on this page, please contact flh.webmaster@dot.gov.