Ambetter Reconsideration Form
Ambetter Reconsideration Form - Web • a request for reconsideration (level i) is a communication from the provider about a disagreement with the manner in which a claim was processed. Web the request for reconsideration/appeal and/or claim dispute must be submitted in writing, which can be mailed, faxed and/or emailed within 365 days from the date on the. Web claims trend form (pdf) provider claims faq (pdf) quality improvement. Web this form may be photocopied required reconsideration/appeal form use this form as part of silversummit healthplan reconsideration/appeal process to address the. All fields are required information. Web inpatient authorization form (pdf) outpatient authorization form (pdf) clinical policy: All fields are required information request for. See coverage in your area; Practice guidelines (pdf) quality improvement (qi) member notification of pregnancy (pdf). • a claim dispute (level.
Web the request for reconsideration/appeal and/or claim dispute must be submitted in writing, which can be mailed, faxed and/or emailed within 365 days from the date on the. All fields are required information. Web provider reconsideration and appeal request form (pdf) covermymeds guide (pdf) update and certify provider data in cms's nppes (pdf) Web provider request for reconsideration and claim dispute form use this form as part of the ambetter from buckeye health plan request for reconsideration. Use your zip code to find your personal plan. All fields are required information a request for. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. See coverage in your area; • a claim dispute (level. Web use this form as part of the ambetter from arkansas health & wellness request for reconsideration and claim dispute process.
Use your zip code to find your personal plan. Web claims trend form (pdf) provider claims faq (pdf) quality improvement. See coverage in your area; Web use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. • a claim dispute (level. All fields are required information a request for reconsideration. All fields are required information request for. Web this form may be photocopied required reconsideration/appeal form use this form as part of silversummit healthplan reconsideration/appeal process to address the. See coverage in your area; All fields are required information a request for.

Reconsideration Vets Disability Guide
Web this form may be photocopied required reconsideration/appeal form use this form as part of silversummit healthplan reconsideration/appeal process to address the. Web claims trend form (pdf) provider claims faq (pdf) quality improvement. Use your zip code to find your personal plan. Web provider reconsideration and appeal request form (pdf) covermymeds guide (pdf) update and certify provider data in cms's.

Gallery of Ambetter Prior Authorization form Beautiful Kircblog 2015
Web provider request for reconsideration and claim dispute form use this form as part of the ambetter from buckeye health plan request for reconsideration. Web • a request for reconsideration (level i) is a communication from the provider about a disagreement with the manner in which a claim was processed. Web the request for reconsideration/appeal and/or claim dispute must be.
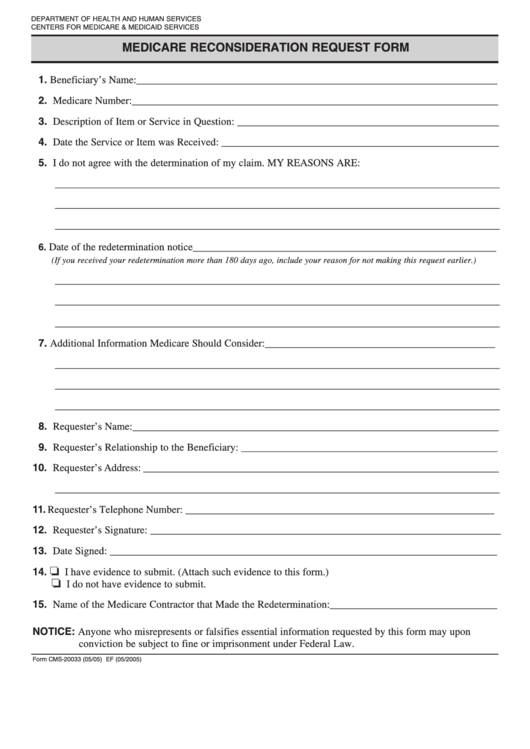
Fillable Medicare Reconsideration Request Form printable pdf download
Web use this form as part of the ambetter of arkansas request for reconsideration and claim dispute process. See coverage in your area; Web the request for reconsideration/appeal and/or claim dispute must be submitted in writing, which can be mailed, faxed and/or emailed within 365 days from the date on the. All fields are required information. Web use this form.
Ambetter Insurance Review My Experience MoneyUnder30
Web use this form as part of the ambetter from meridian request for reconsideration and claim dispute process. Web use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. • a claim dispute (level. All fields are required information. Web this form may be photocopied required reconsideration/appeal form use this form.

Bcbs Appeal Form Texas Fill Online, Printable, Fillable, Blank
• a claim dispute (level. Web inpatient authorization form (pdf) outpatient authorization form (pdf) clinical policy: Web • a request for reconsideration (level i) is a communication from the provider about a disagreement with the manner in which a claim was processed. See coverage in your area; Use your zip code to find your personal plan.

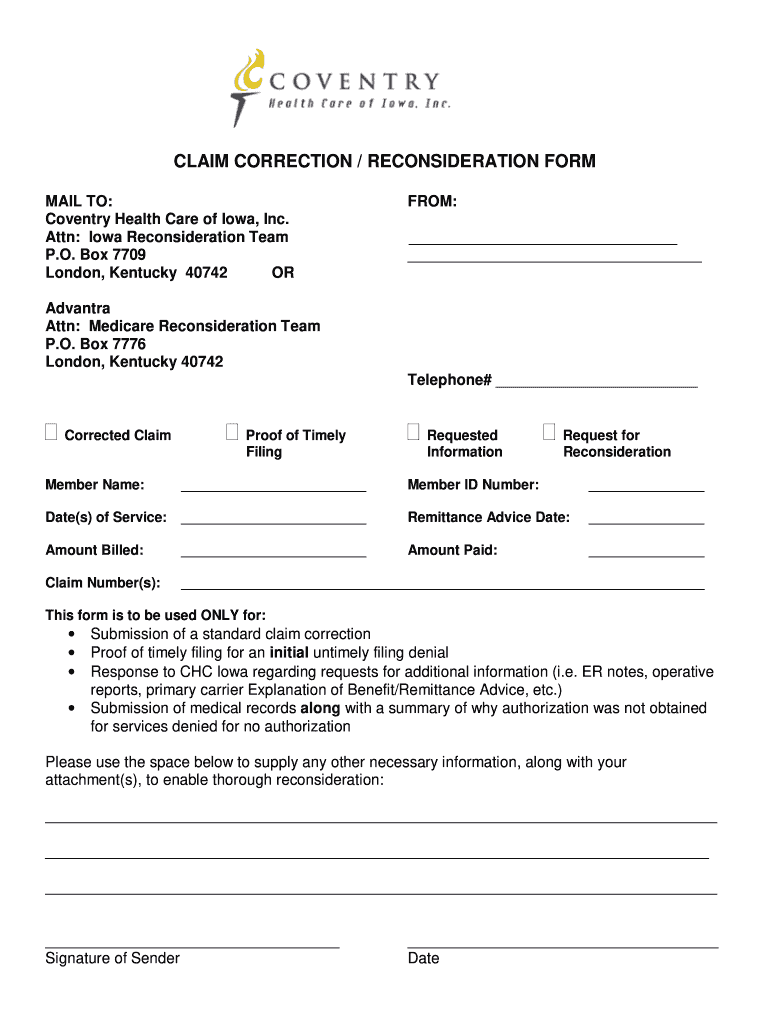
Geisinger Health Plan Request for Claim Reconsideration 20202022
Request for reconsideration and claim dispute process. Web use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. All fields are required information a request for. • a claim dispute (level. Use your zip code to find your personal plan.
Aetna Reconsideration Form Fill Online, Printable, Fillable, Blank
Web provider reconsideration and appeal request form (pdf) covermymeds guide (pdf) update and certify provider data in cms's nppes (pdf) Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. Web use this form as part of the ambetter of arkansas request for reconsideration and claim dispute process. Web inpatient authorization form.

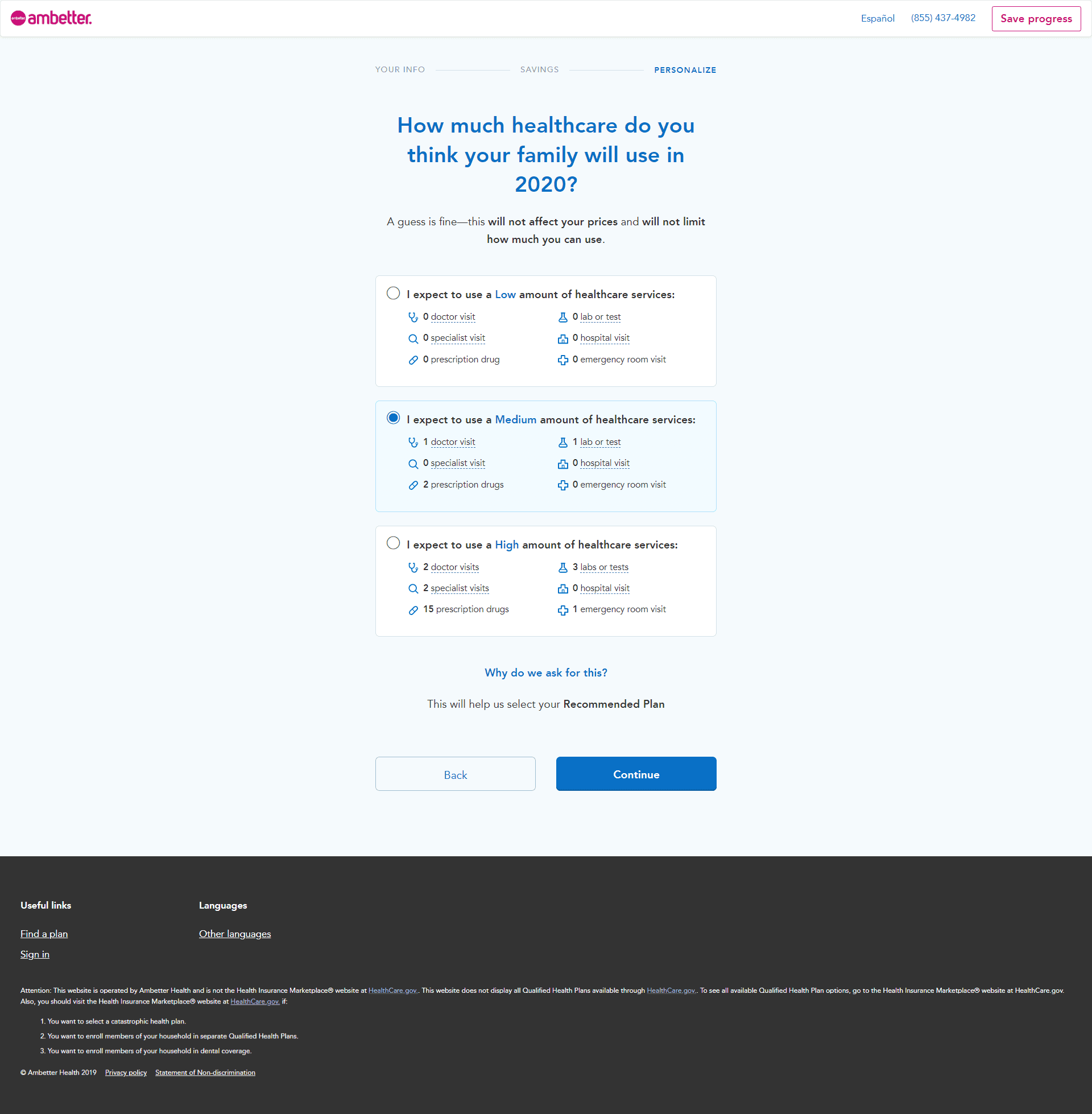
Ambetter Reviews & Ratings
Web use this form as part of the ambetter from meridian request for reconsideration and claim dispute process. Use your zip code to find your personal plan. Web provider request for reconsideration and claim dispute form use this form as part of the ambetter from buckeye health plan request for reconsideration. All fields are required information a request for reconsideration..
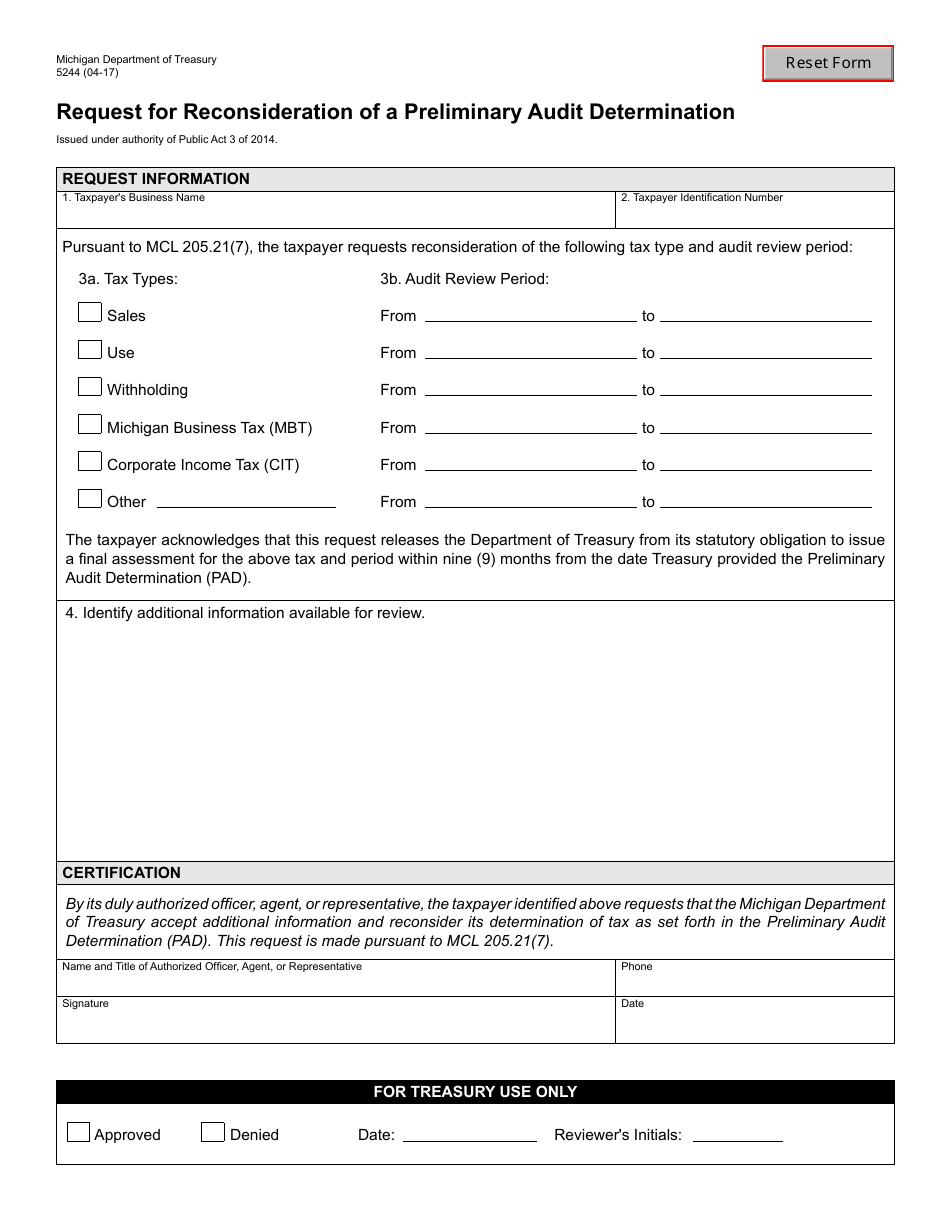
Form 5244 Download Fillable PDF or Fill Online Request for
Request for reconsideration and claim dispute process. All fields are required information request for. Web this form may be photocopied required reconsideration/appeal form use this form as part of silversummit healthplan reconsideration/appeal process to address the. Web use this form as part of the ambetter from home state health request for reconsideration and claim dispute process. • a claim dispute.
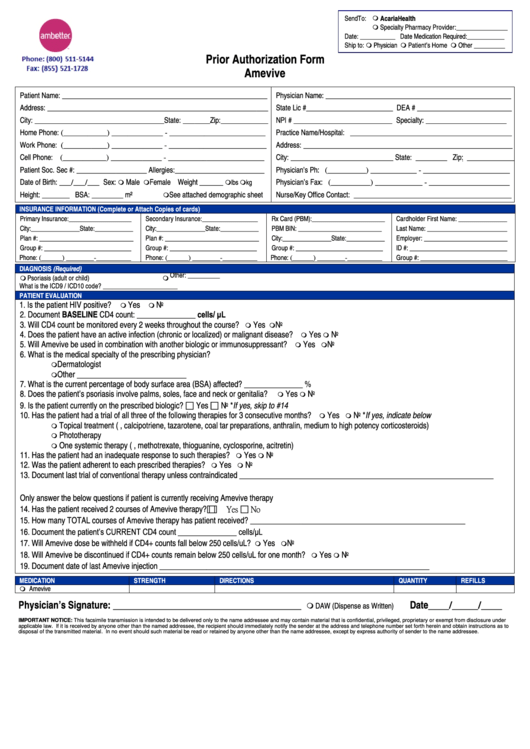
Ambetter Prior Authorization Form Amevive printable pdf download
• a claim dispute (level. Web use this form as part of the ambetter from sunshine health request for reconsideration and claim dispute process. Request for reconsideration and claim dispute process. Web use this form as part of the ambetter of north carolina inc. Web provider reconsideration and appeal request form (pdf) covermymeds guide (pdf) update and certify provider data.
See Coverage In Your Area;
Web inpatient authorization form (pdf) outpatient authorization form (pdf) clinical policy: Use your zip code to find your personal plan. Web the procedures for filing a complaint/grievance or appeal are outlined in the ambetter member’s evidence of coverage. All fields are required information.
Web Provider Request For Reconsideration And Claim Dispute Form Use This Form As Part Of The Ambetter From Buckeye Health Plan Request For Reconsideration.
Web use this form as part of the ambetter from arkansas health & wellness request for reconsideration and claim dispute process. Web use this form as part of the ambetter from meridian request for reconsideration and claim dispute process. Web • a request for reconsideration (level i) is a communication from the provider about a disagreement with the manner in which a claim was processed. All fields are required information request for.
Request For Reconsideration And Claim Dispute Process.
Web claims trend form (pdf) provider claims faq (pdf) quality improvement. All fields are required information a request for reconsideration. All fields are required information a request for. Web use this form as part of the ambetter of north carolina inc.
Web Use This Form As Part Of The Ambetter Of Arkansas Request For Reconsideration And Claim Dispute Process.
Use your zip code to find your personal plan. • a claim dispute (level. Practice guidelines (pdf) quality improvement (qi) member notification of pregnancy (pdf). Web provider reconsideration and appeal request form (pdf) covermymeds guide (pdf) update and certify provider data in cms's nppes (pdf)